

Safety of microneurosurgical interventions for superficial and deep-seated brain metastases: single-center cohort study of 637 consecutive cases
- PMID: 37945819
- PMCID: PMC10689541
- DOI: 10.1007/s11060-023-04478-1
Safety of microneurosurgical interventions for superficial and deep-seated brain metastases: single-center cohort study of 637 consecutive cases
Abstract
Purpose: Microneurosurgical techniques have greatly improved over the past years due to the introduction of new technology and surgical concepts. To reevaluate the role of micro-neurosurgery in brain metastases (BM) resection in the era of new systemic and local treatment options, its safety profile needs to be reassessed. The aim of this study was to analyze the rate of adverse events (AEs) according to a systematic, comprehensive and reliably reproducible grading system after microneurosurgical BM resection in a large and modern microneurosurgical series with special emphasis on anatomical location.
Methods: Prospectively collected cases of BM resection between 2013 and 2022 were retrospectively analyzed. Number of AEs, defined as any deviations from the expected postoperative course according to Clavien-Dindo-Grade (CDG) were evaluated. Patient, surgical, and lesion characteristics, including exact anatomic tumor locations, were analyzed using uni- and multivariate logistic regression and survival analysis to identify predictive factors for AEs.
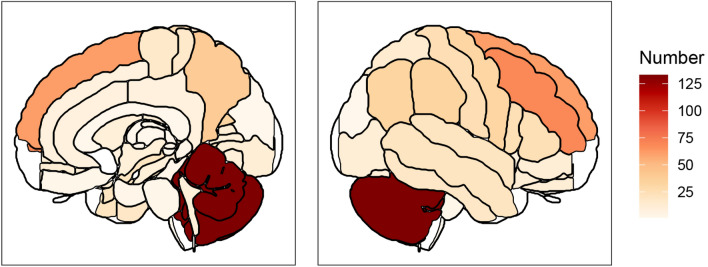
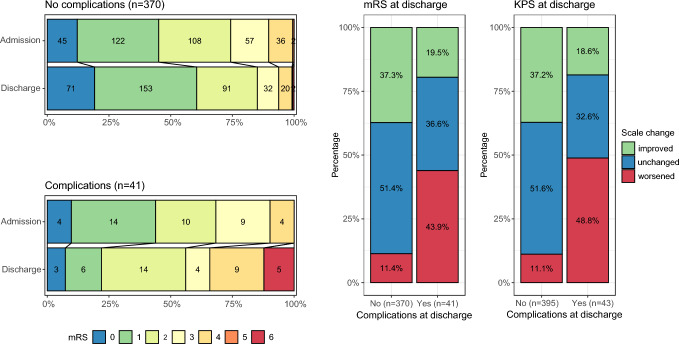
Results: We identified 664 eligible patients with lung cancer being the most common primary tumor (44%), followed by melanoma (25%) and breast cancer (11%). 29 patients (4%) underwent biopsy only whereas BM were resected in 637 (96%) of cases. The overall rate of AEs was 8% at discharge. However, severe AEs (≥ CDG 3a; requiring surgical intervention under local/general anesthesia or ICU treatment) occurred in only 1.9% (n = 12) of cases with a perioperative mortality of 0.6% (n = 4). Infratentorial tumor location (OR 5.46, 95% 2.31-13.8, p = .001), reoperation (OR 2.31, 95% 1.07-4.81, p = .033) and central region tumor location (OR 3.03, 95% 1.03-8.60) showed to be significant predictors in a multivariate analysis for major AEs (CDG ≥ 2 or new neurological deficits). Neither deep supratentorial nor central region tumors were associated with more major AEs compared to convexity lesions.
Conclusions: Modern microneurosurgical resection can be considered an excellent option in the management of BM in terms of safety, as the overall rate of major AEs are very rare even in eloquent and deep-seated lesions.
Keywords: Adverse events; Brain metastases; Complications; Surgical resection.
© 2023. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose
Figures
References
-
- Brastianos PK, Carter SL, Santagata S, et al. Genomic characterization of brain metastases reveals branched evolution and potential therapeutic targets. Cancer Discov. 2015;5:1164–1177. doi: 10.1158/2159-8290.CD-15-0369. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
