

Fracture risk after intralesional curettage of atypical cartilaginous tumors
- PMID: 37946306
- PMCID: PMC10634173
- DOI: 10.1186/s13018-023-04215-4
Fracture risk after intralesional curettage of atypical cartilaginous tumors
Abstract
Introduction: The need for curettage of atypical cartilaginous tumors (ACT) is under debate. Curretage results in defects that weaken the bone potentially leading to fractures. The purpose of this study was to retrospectively determine postoperative fracture risk after curettage of chondroid tumors, including patient-specific characteristics that could influence fracture risk.
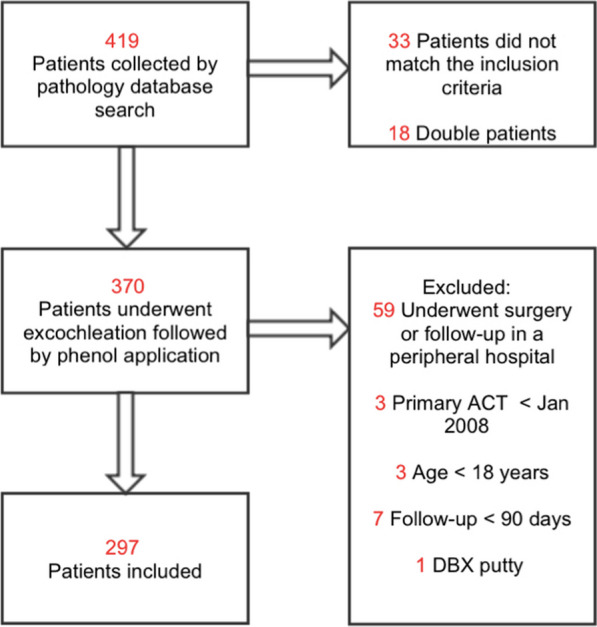
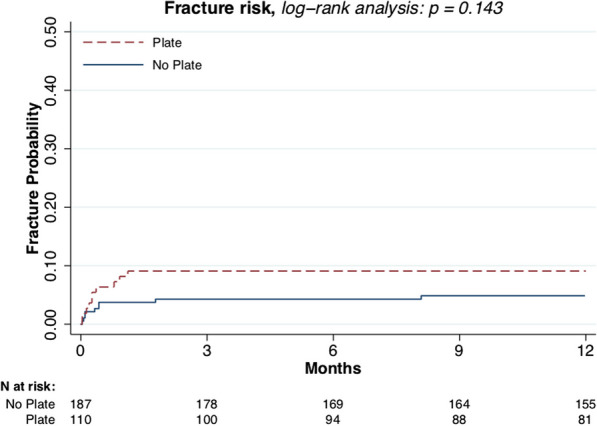
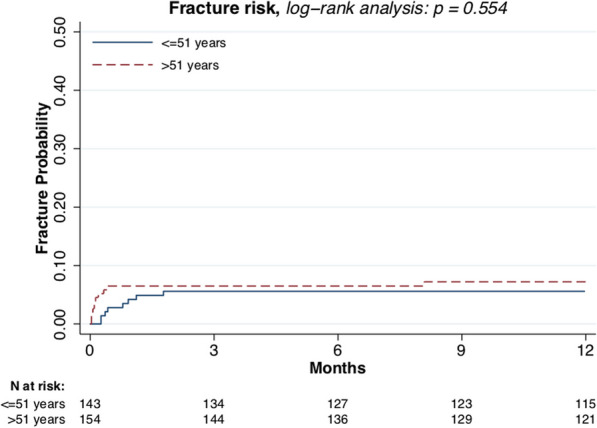
Methods: A total of 297 adult patients who underwent curettage of an ACT followed by phenolisation and augmentation were retrospectively evaluated. Explanatory variables were, sex, age, tumor size, location, augmentation type, and plate fixation. The presence of a postoperative fracture was radiologically diagnosed. Included patients had at least 90 days of follow-up.
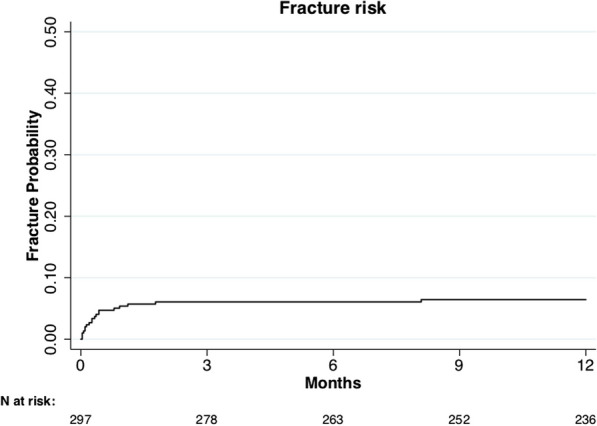
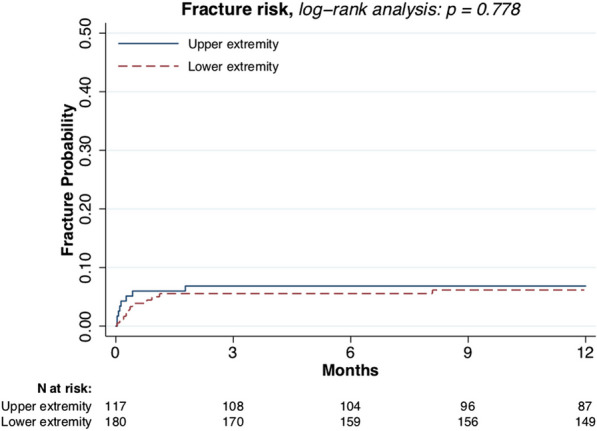
Results: A total of 183 females (62%) were included and 114 males (38%), with an overall median follow-up of 3.2 years (IQR 1.6-5.2). Mean diameter of the lesions was 4.5 (SD 2.8) cm. Patients received augmentation with allograft bone (n = 259, 87%), PMMA (n = 11, 3.7%), or did not receive augmentation (n = 27, 9.1%). Overall fracture risk was 6%. Male sex (p = 0.021) and lesion size larger than 3.8 cm (p < 0.010) were risk factors for postoperative fracture.
Interpretation: Curettage of ACT results in an overall fracture risk of 6%, which is increased for males with larger lesions.
Keywords: ACT; Fracture risk; Orthopedic oncology.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Dierselhuis EF, Gerbers JG, Ploegmakers JJ, Stevens M, Suurmeijer AJ, Jutte PC. Local treatment with adjuvant therapy for central atypical cartilaginous tumors in the long bones: analysis of outcome and complications in one hundred and eight patients with a minimum follow-up of two years. J Bone Jt Surg Am. 2016;98(4):303–313. doi: 10.2106/JBJS.O.00472. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
