

Subclinical Atherosclerosis Across the Menopausal Transition in Women With and Without HIV
- PMID: 37947273
- PMCID: PMC10938198
- DOI: 10.1093/infdis/jiad488
Subclinical Atherosclerosis Across the Menopausal Transition in Women With and Without HIV
Abstract
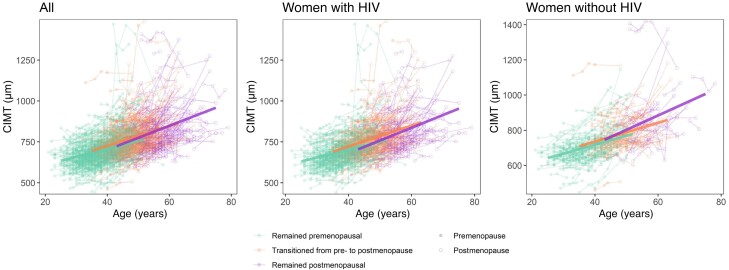
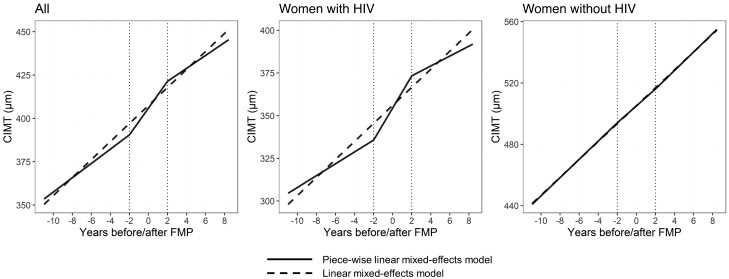
The menopausal transition is a pivotal time of cardiovascular risk, but knowledge is limited in HIV. We studied longitudinal carotid artery intima-media thickness (CIMT) in the Women's Interagency HIV Study (2004-2019; 979 women/3247 person-visits; 72% with HIV). Among women with HIV only, those who transitioned had greater age-related CIMT progression compared to those remaining premenopausal (difference in slope = 1.64 µm/year, P = .002); and CIMT increased over time in the pretransition (3.47 µm/year, P = .002) and during the menopausal transition (9.41 µm/year, P < .0001), but not posttransition (2.9 µm/year, P = .19). In women with HIV, menopause may accelerate subclinical atherosclerosis as measured by CIMT.
Keywords: HIV; atherosclerosis; cardiovascular disease; menopause.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. P. C. T.'s institution has received funding from Merck and Gilead, unrelated to the current manuscript. S. G. K. has developed educational materials related to HIV with Integritas Communications, LLC and Vindico CME. A. S. has received grant funding from Gilead Sciences, Inc, outside the submitted work. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- El Khoudary SR, Aggarwal B, Beckie TM, et al. Menopause transition and cardiovascular disease risk: implications for timing of early prevention: a scientific statement from the American Heart Association. Circulation 2020; 142:e506–32. - PubMed
Publication types
MeSH terms
Grants and funding
- P30 AI027767/AI/NIAID NIH HHS/United States
- P30 AI050409/AI/NIAID NIH HHS/United States
- MD/NIMHD NIH HHS/United States
- U01 HL146245/HL/NHLBI NIH HHS/United States
- AA/NIAAA NIH HHS/United States
- K01HL160146/HL/NHLBI NIH HHS/United States
- KL2 TR001432/TR/NCATS NIH HHS/United States
- U01 HL146242/HL/NHLBI NIH HHS/United States
- K23 AG084415/AG/NIA NIH HHS/United States
- TL1 TR001431/TR/NCATS NIH HHS/United States
- U01 HL146241/HL/NHLBI NIH HHS/United States
- CA/NCI NIH HHS/United States
- R01 HL148094/HL/NHLBI NIH HHS/United States
- DK/NIDDK NIH HHS/United States
- DA/NIDA NIH HHS/United States
- DC/NIDCD NIH HHS/United States
- DE/NIDCR NIH HHS/United States
- U01 HL146194/HL/NHLBI NIH HHS/United States
- NR/NINR NIH HHS/United States
- P30 MH116867/MH/NIMH NIH HHS/United States
- U01 HL146205/HL/NHLBI NIH HHS/United States
- UL1 TR001409/TR/NCATS NIH HHS/United States
- K01 HL160146/HL/NHLBI NIH HHS/United States
- U01 HL146333/HL/NHLBI NIH HHS/United States
- U01 HL146240/HL/NHLBI NIH HHS/United States
- P30 AI073961/AI/NIAID NIH HHS/United States
- NS/NINDS NIH HHS/United States
- U01 HL146192/HL/NHLBI NIH HHS/United States
- R01 HL140976/HL/NHLBI NIH HHS/United States
- L30 HL159721/HL/NHLBI NIH HHS/United States
- U01 HL146208/HL/NHLBI NIH HHS/United States
- U01 HL146204/HL/NHLBI NIH HHS/United States
- U01 HL146193/HL/NHLBI NIH HHS/United States
- U01 HL146202/HL/NHLBI NIH HHS/United States
- U01 HL146201/HL/NHLBI NIH HHS/United States
- U01 HL146203/HL/NHLBI NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- UL1 TR000004/TR/NCATS NIH HHS/United States
- K01 HL137557/HL/NHLBI NIH HHS/United States
- UL1 TR003098/TR/NCATS NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
