

The Influence of Potential Organ Donors on Standardized Mortality Ratios and ICU Benchmarking
- PMID: 37947476
- PMCID: PMC10876165
- DOI: 10.1097/CCM.0000000000006098
The Influence of Potential Organ Donors on Standardized Mortality Ratios and ICU Benchmarking
Abstract
Objectives: The standardized mortality ratio (SMR) is a common metric to benchmark ICUs. However, SMR may be artificially distorted by the admission of potential organ donors (POD), who have nearly 100% mortality, although risk prediction models may not identify them as high-risk patients. We aimed to evaluate the impact of PODs on SMR.
Design: Retrospective registry-based multicenter study.
Setting: Twenty ICUs in Finland, Estonia, and Switzerland in 2015-2017.
Patients: Sixty thousand forty-seven ICU patients.
Interventions: None.
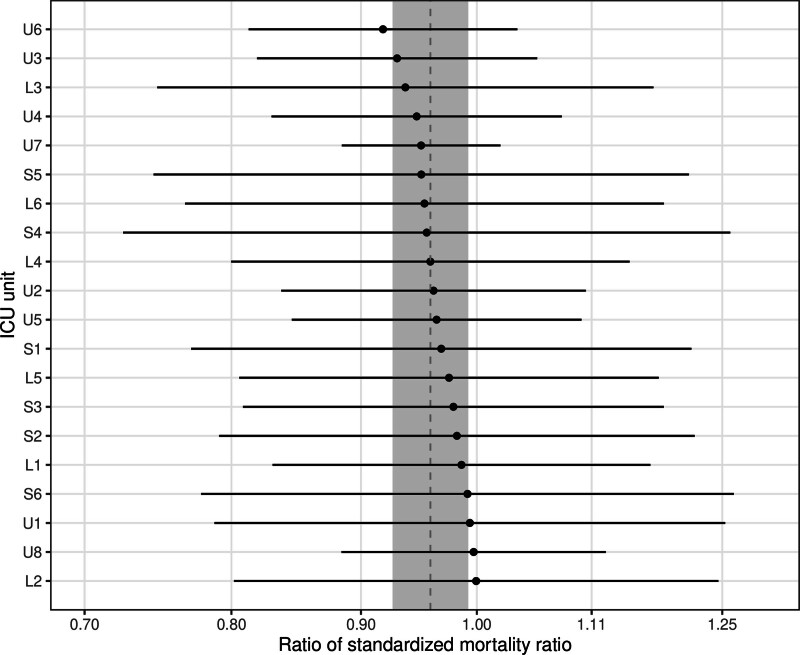
Measurements and main results: We used a previously validated mortality risk model to calculate the SMRs. We investigated the impact of PODs on the overall SMR, individual ICU SMR and ICU benchmarking. Of the 60,047 patients admitted to the ICUs, 514 (0.9%) were PODs, and 477 (93%) of them died. POD deaths accounted for 7% of the total 6738 in-hospital deaths. POD admission rates varied from 0.5 to 18.3 per 1000 admissions across ICUs. The risk prediction model predicted a 39% in-hospital mortality for PODs, but the observed mortality was 93%. The ratio of the SMR of the cohort without PODs to the SMR of the cohort with PODs was 0.96 (95% CI, 0.93-0.99). Benchmarking results changed in 70% of ICUs after excluding PODs.
Conclusions: Despite their relatively small overall number, PODs make up a large proportion of ICU patients who die. PODs cause bias in SMRs and in ICU benchmarking. We suggest excluding PODs when benchmarking ICUs with SMR.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and Wolters Kluwer Health, Inc.
Conflict of interest statement
Dr. Pölkki was supported by institutional funding from Kuopio University Hospital, University of Eastern Finland, and The Finnish Society of Anaesthesiologists. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures


Comment in
-
The Standardized Mortality Ratio and ICU Benchmarking: An Old Measure That Is Still Missing the Mark.Crit Care Med. 2024 Mar 1;52(3):498-501. doi: 10.1097/CCM.0000000000006109. Epub 2024 Feb 21. Crit Care Med. 2024. PMID: 38381010 No abstract available.
-
Case-Mix and the Limitations of Standardized Mortality Ratios for ICU Performance and Benchmarking.Crit Care Med. 2024 Apr 1;52(4):e216-e217. doi: 10.1097/CCM.0000000000006183. Epub 2024 Mar 14. Crit Care Med. 2024. PMID: 38483238 No abstract available.
References
-
- Salluh JIF, Soares M, Keegan MT: Understanding intensive care unit benchmarking. Intensive Care Med. 2017; 43:1703–1707 - PubMed
-
- Zimmerman JE, Kramer AA, McNair DS, et al. : Acute Physiology and Chronic Health Evaluation (APACHE) IV: Hospital mortality assessment for today’s critically ill patients. Crit Care Med. 2006; 34:1297–1310 - PubMed
-
- Higgins T, Teres D, Nathanson B, et al. : Updated mortality probability model - MPM0-III. Chest. 2005; 128(4 Suppl):348S–348S
