

Immersive virtual reality-based rehabilitation for subacute stroke: a randomized controlled trial
- PMID: 37947856
- PMCID: PMC10896795
- DOI: 10.1007/s00415-023-12060-y
Immersive virtual reality-based rehabilitation for subacute stroke: a randomized controlled trial
Abstract
Objective: Few effective treatments improve upper extremity (UE) function after stroke. Immersive virtual reality (imVR) is a novel and promising strategy for stroke UE recovery. We assessed the extent to which imVR-based UE rehabilitation can augment conventional treatment and explored changes in brain functional connectivity (FC) that were related to the rehabilitation.
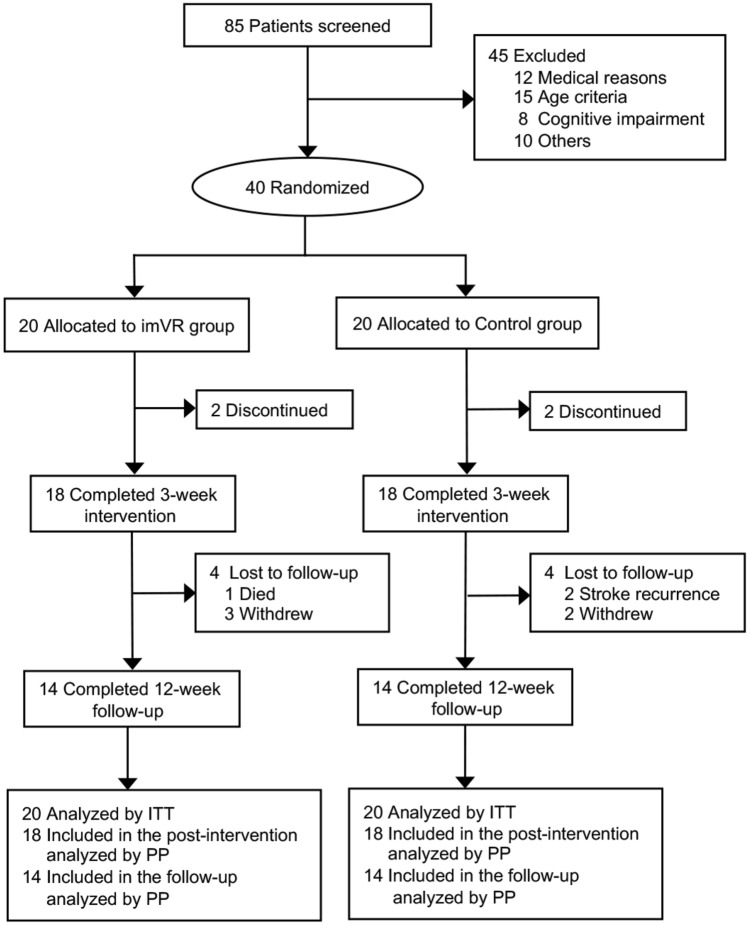
Methods: An assessor-blinded, parallel-group randomized controlled trial was performed with 40 subjects randomly assigned to either imVR or Control group (1:1 allocation), each receiving rehabilitation 5 times per week for 3 weeks. Subjects in the imVR received both imVR and conventional rehabilitation, while those in the Control received conventional rehabilitation only. Our primary and secondary outcomes were the Fugl-Meyer assessment's upper extremity subscale (FMA-UE) and the Barthel Index (BI), respectively. Both intention-to-treat (ITT) and per-protocol (PP) analyses were performed to assess the effectiveness of the trial. For both the FMA-UE/BI, a one-way analysis of covariance (ANCOVA) model was used, with the FMA-UE/BI at post-intervention or at follow-up, respectively, as the dependent variable, the two groups as the independent variable, baseline FMA-UE/BI, age, sex, site, time since onset, hypertension and diabetes as covariates.
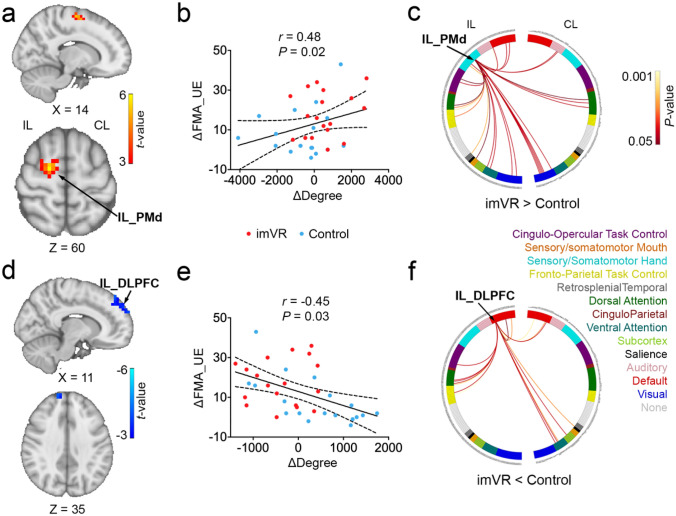
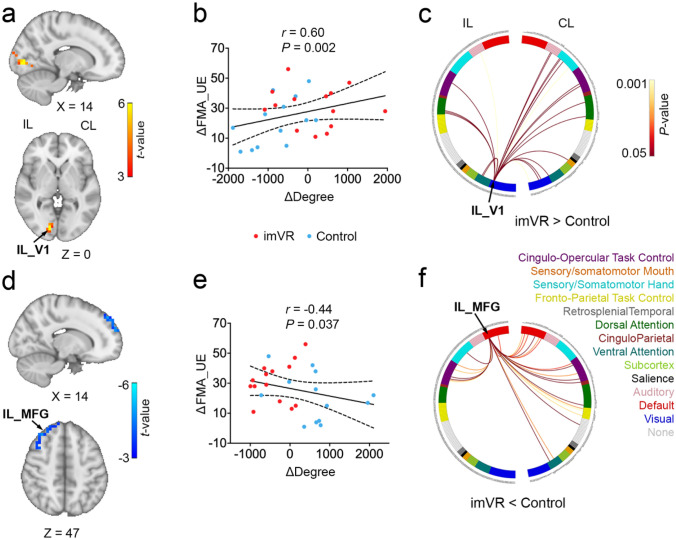
Results: Both ITT and PP analyses demonstrated the effectiveness of imVR-based rehabilitation. The FMA-UE score was greater in the imVR compared with the Control at the post-intervention (mean difference: 9.1 (95% CI 1.6, 16.6); P = 0.019) and follow-up (mean difference:11.5 (95% CI 1.9, 21.0); P = 0.020). The results were consistent for BI scores. Moreover, brain FC analysis found that the motor function improvements were associated with a change in degree in ipsilesional premotor cortex and ipsilesional dorsolateral prefrontal cortex immediately following the intervention and in ipsilesional visual region and ipsilesional middle frontal gyrus after the 12-week follow-up.
Conclusions: ImVR-based rehabilitation is an effective tool that can improve the recovery of UE functional capabilities of subacute stroke patients when added to standard care. These improvements were associated with distinctive brain changes at two post-stroke timepoints. The study results will benefit future patients with stroke and provide evidence for a promising new method of stroke rehabilitation.
Trial registration: ClinicalTrials.gov identifier: NCT03086889.
Keywords: Brain functional connectivity; Functional magnetic resonance imaging; Immersive virtual reality rehabilitation; Stroke.
© 2023. The Author(s).
Conflict of interest statement
The authors report no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
