

Ambulatory Intensive Care for Medically Complex Patients at a Health Care Clinic for Individuals Experiencing Homelessness: The SUMMIT Randomized Clinical Trial
- PMID: 37948081
- PMCID: PMC10638646
- DOI: 10.1001/jamanetworkopen.2023.42012
Ambulatory Intensive Care for Medically Complex Patients at a Health Care Clinic for Individuals Experiencing Homelessness: The SUMMIT Randomized Clinical Trial
Abstract
Importance: Intensive primary care interventions have been promoted to reduce hospitalization rates and improve health outcomes for medically complex patients, but evidence of their efficacy is limited.
Objective: To assess the efficacy of a multidisciplinary ambulatory intensive care unit (A-ICU) intervention on health care utilization and patient-reported outcomes.
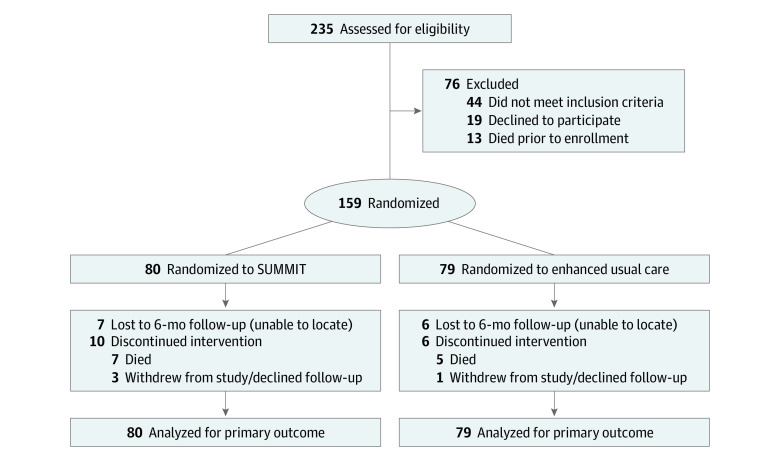
Design, setting, and participants: The Streamlined Unified Meaningfully Managed Interdisciplinary Team (SUMMIT) randomized clinical trial used a wait-list control design and was conducted at a health care clinic for patients experiencing homelessness in Portland, Oregon. The first patient was enrolled in August 2016, and the last patient was enrolled in November 2019. Included patients had 1 or more hospitalizations in the prior 6 months and 2 or more chronic medical conditions, substance use disorder, or mental illness. Data analysis was performed between March and May 2021.
Intervention: The A-ICU included a team manager, a pharmacist, a nurse, care coordinators, social workers, and physicians. Activities included comprehensive 90-minute intake, transitional care coordination, and flexible appointments, with reduced panel size. Enhanced usual care (EUC), consisting of team-based primary care with access to community health workers and mental health, addiction treatment, and pharmacy services, served as the comparator. Participants who received EUC joined the A-ICU intervention after 6 months.
Main outcomes and measures: The main outcome was the difference in rates of hospitalization (primary outcome), emergency department (ED) visits, and primary care physician (PCP) visits per person over 6 months (vs the prior 6 months). Patient-reported outcomes included changes in patient activation, experience, health-related quality of life, and self-rated health at 6 months (vs baseline). We performed an intention-to-treat analysis using a linear mixed-effects model with a random intercept for each patient to examine the association between study group and outcomes.
Results: This study randomized 159 participants (mean [SD] age, 54.9 [9.8] years) to the A-ICU SUMMIT intervention (n = 80) or to EUC (n = 79). The majority of participants were men (102 [65.8%]) and most were White (121 [76.1%]). A total of 64 participants (41.0%) reported having unstable housing at baseline. Six-month hospitalizations decreased in both the A-ICU and EUC groups, with no difference between them (mean [SE], -0.6 [0.5] vs -0.9 [0.5]; difference, 0.3 [95% CI, -1.0 to 1.5]). Emergency department use did not differ between groups (mean [SE], -2.0 [1.0] vs 0.9 [1.0] visits per person; difference, -1.1 [95% CI, -3.7 to 1.6]). Primary care physician visits increased in the A-ICU group (mean [SE], 4.2 [1.6] vs -2.0 [1.6] per person; difference, 6.1 [95% CI, 1.8 to 10.4]). Patients in the A-ICU group reported improved social functioning (mean [SE], 4.7 [2.0] vs -1.1 [2.0]; difference, 5.8 [95% CI, 0.3 to 11.2]) and self-rated health (mean [SE], 0.7 [0.3] vs -0.2 [0.3]; difference, 1.0 [95% CI, 0.1 to 1.8]) compared with patients in the EUC group. No differences in patient activation or experience were observed.
Conclusions and relevance: The A-ICU intervention did not change hospital or ED utilization at 6 months but increased PCP visits and improved patient well-being. Longer-term studies are needed to evaluate whether these observed improvements lead to eventual changes in acute care utilization.
Trial registration: ClinicalTrials.gov Identifier: NCT03224858.
Conflict of interest statement
Figures
Similar articles
-
The SUMMIT ambulatory-ICU primary care model for medically and socially complex patients in an urban federally qualified health center: study design and rationale.Addict Sci Clin Pract. 2018 Dec 14;13(1):27. doi: 10.1186/s13722-018-0128-y. Addict Sci Clin Pract. 2018. PMID: 30547847 Free PMC article.
-
Helping Patients with COPD Transition from Hospital to Home—The BREATHE Study [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2020 Apr. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2020 Apr. PMID: 39680694 Free Books & Documents. Review.
-
Effect of a housing and case management program on emergency department visits and hospitalizations among chronically ill homeless adults: a randomized trial.JAMA. 2009 May 6;301(17):1771-8. doi: 10.1001/jama.2009.561. JAMA. 2009. PMID: 19417194 Clinical Trial.
-
Effect of a Coordinated Community and Chronic Care Model Team Intervention vs Usual Care on Systolic Blood Pressure in Patients With Stroke or Transient Ischemic Attack: The SUCCEED Randomized Clinical Trial.JAMA Netw Open. 2021 Feb 1;4(2):e2036227. doi: 10.1001/jamanetworkopen.2020.36227. JAMA Netw Open. 2021. PMID: 33587132 Free PMC article. Clinical Trial.
-
A comprehensive review of prioritised interventions to improve the health and wellbeing of persons with lived experience of homelessness.Campbell Syst Rev. 2021 Jun 24;17(2):e1154. doi: 10.1002/cl2.1154. eCollection 2021 Jun. Campbell Syst Rev. 2021. Update in: Campbell Syst Rev. 2019 Sep 12;15(3):e1048. doi: 10.1002/cl2.1048. PMID: 37131928 Free PMC article. Updated. Review.
Cited by
-
Onsite Primary Care to Address Medical Needs Among Permanent Supportive Housing Tenants: A Feasibility Demonstration Project.J Gen Intern Med. 2025 May;40(7):1545-1549. doi: 10.1007/s11606-024-09256-x. Epub 2025 Jan 14. J Gen Intern Med. 2025. PMID: 39809961
-
Are tailored primary care services for social inclusion good value for money? A health economics evaluation with Monte-Carlo probabilistic sensitivity analysis comparing tailored social inclusion primary care services to mainstream primary care services for socially excluded people.Int J Equity Health. 2025 May 31;24(1):159. doi: 10.1186/s12939-025-02532-0. Int J Equity Health. 2025. PMID: 40450282 Free PMC article.
-
Geriatrics-Focused vs Traditional Primary Care in the Veterans Affairs Health Care System.JAMA Netw Open. 2025 Jan 2;8(1):e2454865. doi: 10.1001/jamanetworkopen.2024.54865. JAMA Netw Open. 2025. PMID: 39820691 Free PMC article.
-
Interprofessional collaboration between pharmacists and community health workers: a scoping review.Int J Equity Health. 2025 Jan 21;24(1):23. doi: 10.1186/s12939-025-02377-7. Int J Equity Health. 2025. PMID: 39838436 Free PMC article.
-
Health Care Models for Persons with Multiple Chronic Conditions from Populations that Experience Health Disparities: A Scoping Review.J Gen Intern Med. 2025 Jul;40(10):2346-2357. doi: 10.1007/s11606-025-09491-w. Epub 2025 Apr 23. J Gen Intern Med. 2025. PMID: 40268836 Free PMC article. Review.
References
-
- Government Accountability Office . Medicaid: A Small Share of Enrollees Consistently Accounted for a Large Share of Expenditures. Report No. GAO-15-460. US Government Printing Office; 2015.
-
- National Association of Community Health Centers . Community Health Center Chartbook. Accessed January 25, 2022. https://www.nachc.org/resource/community-health-center-chartbook-2022/
