

MiR-326-mediated overexpression of NFIB offsets TGF-β induced epithelial to mesenchymal transition and reverses lung fibrosis
- PMID: 37950757
- PMCID: PMC11072886
- DOI: 10.1007/s00018-023-05005-1
MiR-326-mediated overexpression of NFIB offsets TGF-β induced epithelial to mesenchymal transition and reverses lung fibrosis
Abstract
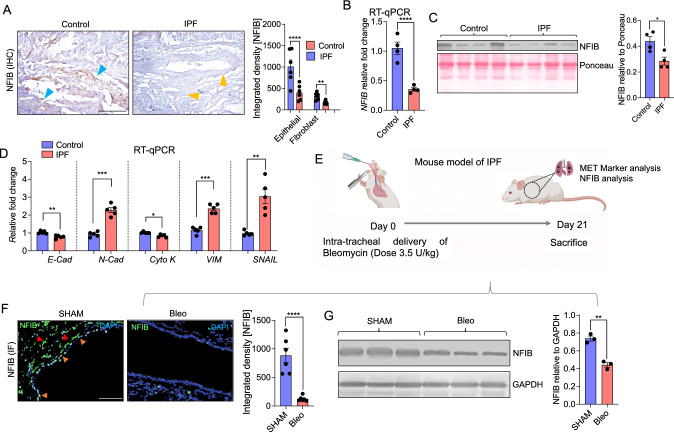
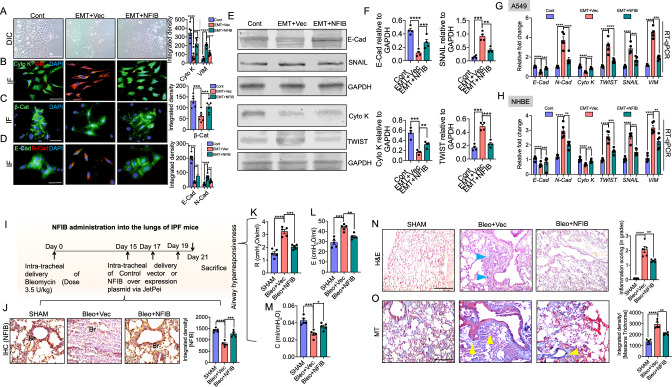
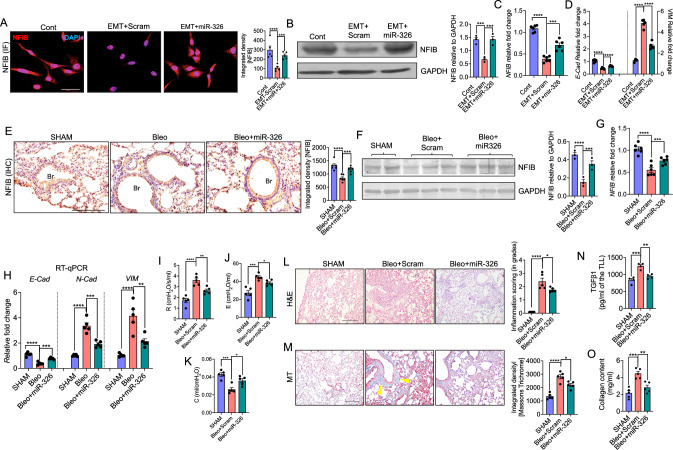
Idiopathic Pulmonary Fibrosis (IPF) is a progressively fatal and incurable disease characterized by the loss of alveolar structures, increased epithelial-mesenchymal transition (EMT), and aberrant tissue repair. In this study, we investigated the role of Nuclear Factor I-B (NFIB), a transcription factor critical for lung development and maturation, in IPF. Using both human lung tissue samples from patients with IPF, and a mouse model of lung fibrosis induced by bleomycin, we showed that there was a significant reduction of NFIB both in the lungs of patients and mice with IPF. Furthermore, our in vitro experiments using cultured human lung cells demonstrated that the loss of NFIB was associated with the induction of EMT by transforming growth factor beta (TGF-β). Knockdown of NFIB promoted EMT, while overexpression of NFIB suppressed EMT and attenuated the severity of bleomycin-induced lung fibrosis in mice. Mechanistically, we identified post-translational regulation of NFIB by miR-326, a miRNA with anti-fibrotic effects that is diminished in IPF. Specifically, we showed that miR-326 stabilized and increased the expression of NFIB through its 3'UTR target sites for Human antigen R (HuR). Moreover, treatment of mice with either NFIB plasmid or miR-326 reversed airway collagen deposition and fibrosis. In conclusion, our study emphasizes the critical role of NFIB in lung development and maturation, and its reduction in IPF leading to EMT and loss of alveolar structures. Our study highlights the potential of miR-326 as a therapeutic intervention for IPF. The schema shows the role of NFIB in maintaining the normal epithelial cell characteristics in the lungs and how its reduction leads to a shift towards mesenchymal cell-like features and pulmonary fibrosis. A In normal lungs, NFIB is expressed abundantly in the epithelial cells, which helps in maintaining their shape, cell polarity and adhesion molecules. However, when the lungs are exposed to factors that induce pulmonary fibrosis, such as bleomycin, or TGF-β, the epithelial cells undergo epithelial to mesenchymal transition (EMT), which leads to a decrease in NFIB. B The mesenchymal cells that arise from EMT appear as spindle-shaped with loss of cell junctions, increased cell migration, loss of polarity and expression of markers associated with mesenchymal cells/fibroblasts. C We designed a therapeutic approach that involves exogenous administration of NFIB in the form of overexpression plasmid or microRNA-326. This therapeutic approach decreases the mesenchymal cell phenotype and restores the epithelial cell phenotype, thus preventing the development or progression of pulmonary fibrosis.
Keywords: Epithelial–mesenchymal transition; Idiopathic pulmonary fibrosis; NFIB; miR-326.
© 2023. The Author(s), under exclusive licence to Springer Nature Switzerland AG.
Conflict of interest statement
The authors declare that they have no competing interests pertaining to this work.
Figures


References
-
- Pardo A, Selman M, Kaminski N. Approaching the degradome in idiopathic pulmonary fibrosis. Int J Biochem Cell Biol. 2008;40(6–7):1141–1155. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
