

Device-measured physical activity and cardiometabolic health: the Prospective Physical Activity, Sitting, and Sleep (ProPASS) consortium
- PMID: 37950859
- PMCID: PMC10849343
- DOI: 10.1093/eurheartj/ehad717
Device-measured physical activity and cardiometabolic health: the Prospective Physical Activity, Sitting, and Sleep (ProPASS) consortium
Abstract
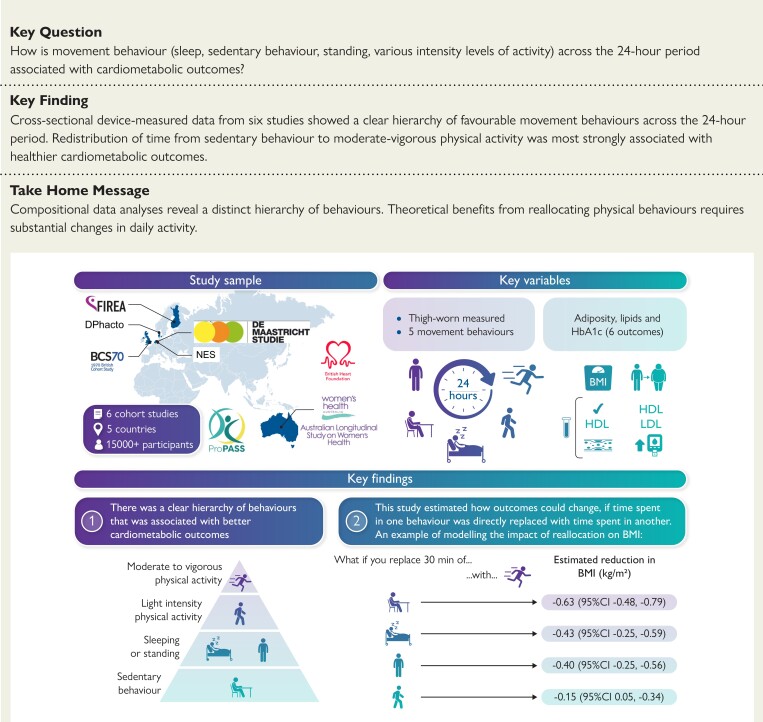
Background and aims: Physical inactivity, sedentary behaviour (SB), and inadequate sleep are key behavioural risk factors of cardiometabolic diseases. Each behaviour is mainly considered in isolation, despite clear behavioural and biological interdependencies. The aim of this study was to investigate associations of five-part movement compositions with adiposity and cardiometabolic biomarkers.
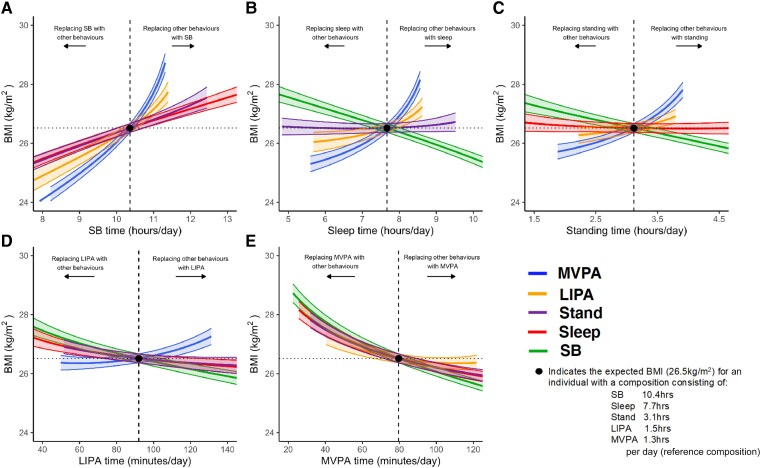
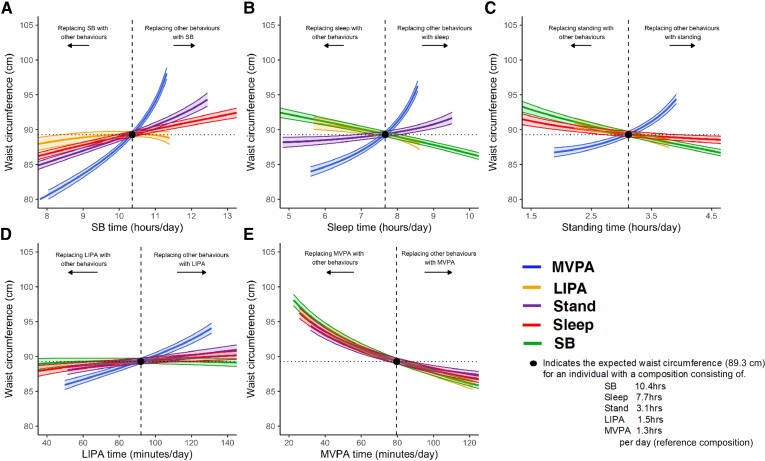
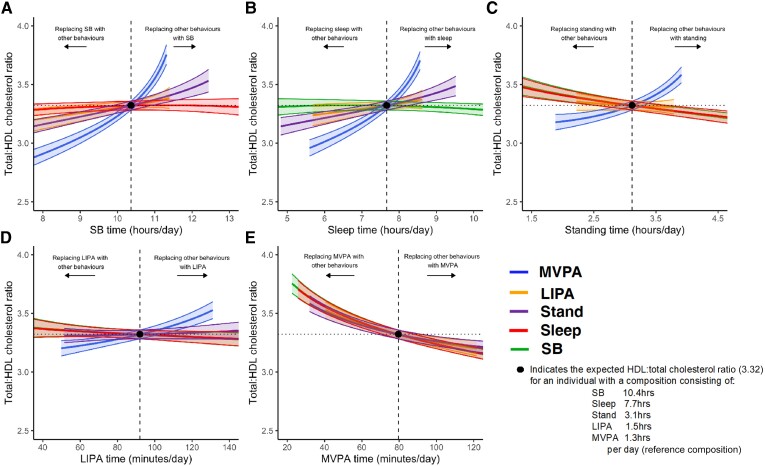
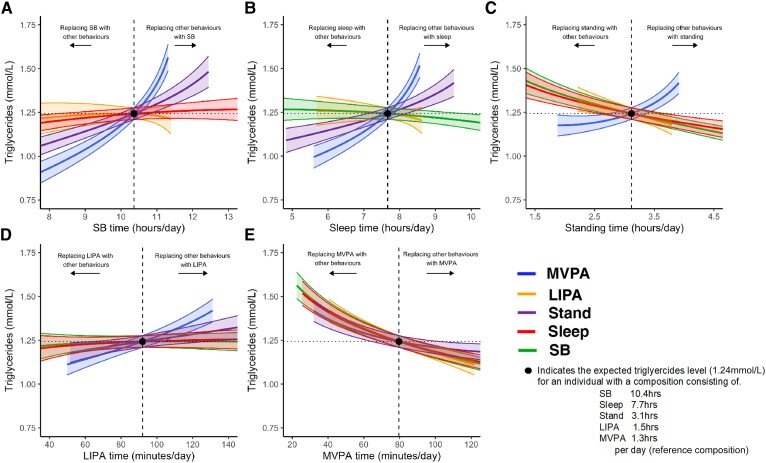
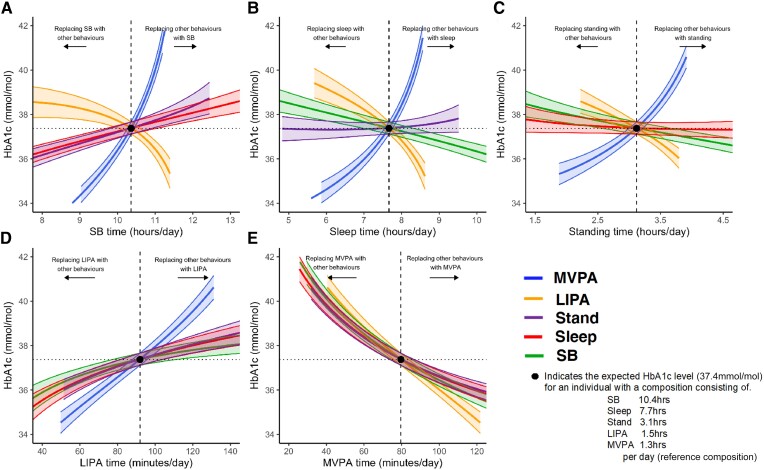
Methods: Cross-sectional data from six studies (n = 15 253 participants; five countries) from the Prospective Physical Activity, Sitting and Sleep consortium were analysed. Device-measured time spent in sleep, SB, standing, light-intensity physical activity (LIPA), and moderate-vigorous physical activity (MVPA) made up the composition. Outcomes included body mass index (BMI), waist circumference, HDL cholesterol, total:HDL cholesterol ratio, triglycerides, and glycated haemoglobin (HbA1c). Compositional linear regression examined associations between compositions and outcomes, including modelling time reallocation between behaviours.
Results: The average daily composition of the sample (age: 53.7 ± 9.7 years; 54.7% female) was 7.7 h sleeping, 10.4 h sedentary, 3.1 h standing, 1.5 h LIPA, and 1.3 h MVPA. A greater MVPA proportion and smaller SB proportion were associated with better outcomes. Reallocating time from SB, standing, LIPA, or sleep into MVPA resulted in better scores across all outcomes. For example, replacing 30 min of SB, sleep, standing, or LIPA with MVPA was associated with -0.63 (95% confidence interval -0.48, -0.79), -0.43 (-0.25, -0.59), -0.40 (-0.25, -0.56), and -0.15 (0.05, -0.34) kg/m2 lower BMI, respectively. Greater relative standing time was beneficial, whereas sleep had a detrimental association when replacing LIPA/MVPA and positive association when replacing SB. The minimal displacement of any behaviour into MVPA for improved cardiometabolic health ranged from 3.8 (HbA1c) to 12.7 (triglycerides) min/day.
Conclusions: Compositional data analyses revealed a distinct hierarchy of behaviours. Moderate-vigorous physical activity demonstrated the strongest, most time-efficient protective associations with cardiometabolic outcomes. Theoretical benefits from reallocating SB into sleep, standing, or LIPA required substantial changes in daily activity.
Keywords: Cardiometabolic outcomes; Cohort consortium; Compositional data analysis; Physical activity; Sedentary behaviour; Sleep; Standing.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

Comment in
-
Balancing our day for heart health.Eur Heart J. 2024 Feb 7;45(6):472-474. doi: 10.1093/eurheartj/ehad824. Eur Heart J. 2024. PMID: 38103181 No abstract available.
References
-
- World Health Organisation . Cardiovascular diseases (CVDs) factsheet. https://www.who.int/en/news-room/fact-sheets/detail/cardiovascular-disea....
