

Prerequisites to improve surgical cytoreduction in FIGO stage III/IV epithelial ovarian cancer and subsequent clinical ramifications
- PMID: 37951927
- PMCID: PMC10638711
- DOI: 10.1186/s13048-023-01303-1
Prerequisites to improve surgical cytoreduction in FIGO stage III/IV epithelial ovarian cancer and subsequent clinical ramifications
Abstract
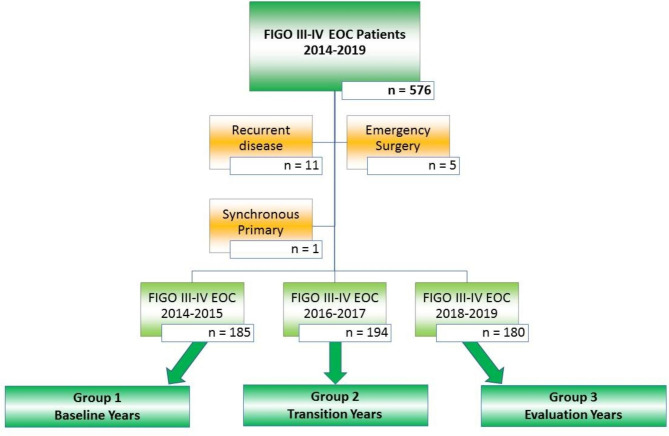
Background: No residual disease (CC 0) following cytoreductive surgery is pivotal for the prognosis of women with advanced stage epithelial ovarian cancer (EOC). Improving CC 0 resection rates without increasing morbidity and no delay in subsequent chemotherapy favors a better outcome in these women. Prerequisites to facilitate this surgical paradigm shift and subsequent ramifications need to be addressed. This quality improvement study assessed 559 women with advanced EOC who had cytoreductive surgery between January 2014 and December 2019 in our tertiary referral centre. Following implementation of the Enhanced Recovery After Surgery (ERAS) pathway and prehabilitation protocols, the surgical management paradigm in advanced EOC patients shifted towards maximal surgical effort cytoreduction in 2016. Surgical outcome parameters before, during, and after this paradigm shift were compared. The primary outcome measure was residual disease (RD). The secondary outcome parameters were postoperative morbidity, operative time (OT), length of stay (LOS) and progression-free-survival (PFS).
Results: R0 resection rate in patients with advanced EOC increased from 57.3% to 74.4% after the paradigm shift in surgical management whilst peri-operative morbidity and delays in adjuvant chemotherapy were unchanged. The mean OT increased from 133 + 55 min to 197 + 85 min, and postoperative high dependency/intensive care unit (HDU/ICU) admissions increased from 8.1% to 33.1%. The subsequent mean LOS increased from 7.0 + 2.6 to 8.4 + 4.9 days. The median PFS was 33 months. There was no difference for PFS in the three time frames but a trend towards improvement was observed.
Conclusions: Improved CC 0 surgical cytoreduction rates without compromising morbidity in advanced EOC is achievable owing to the right conditions. Maximal effort cytoreductive surgery should solely be carried out in high output tertiary referral centres due to the associated substantial prerequisites and ramifications.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Griffiths CT. Surgical resection of Tumor bulk in the primary treatment of ovarian carcinoma. Natl Cancer Inst Monogr. 1975;42:101–4. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
