

Dostarlimab or pembrolizumab plus chemotherapy in previously untreated metastatic non-squamous non-small cell lung cancer: the randomized PERLA phase II trial
- PMID: 37951954
- PMCID: PMC10640551
- DOI: 10.1038/s41467-023-42900-4
Dostarlimab or pembrolizumab plus chemotherapy in previously untreated metastatic non-squamous non-small cell lung cancer: the randomized PERLA phase II trial
Abstract
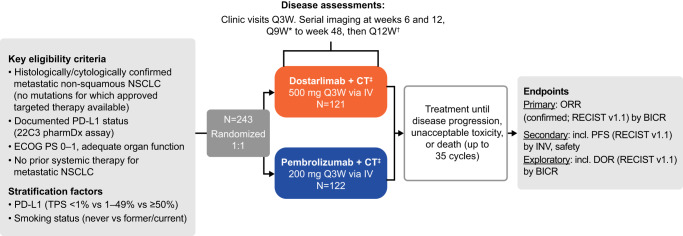
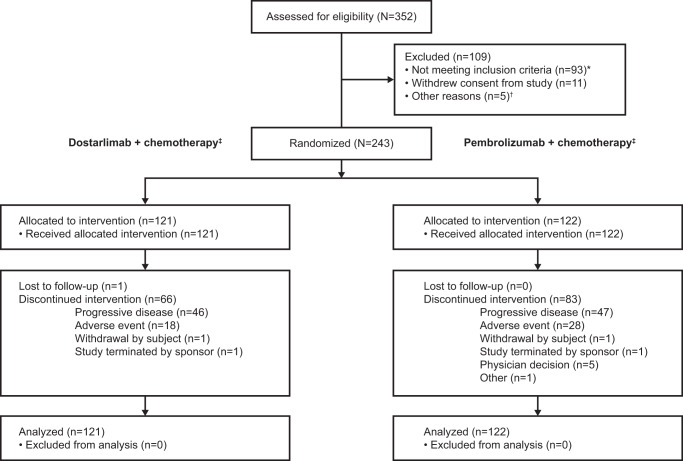
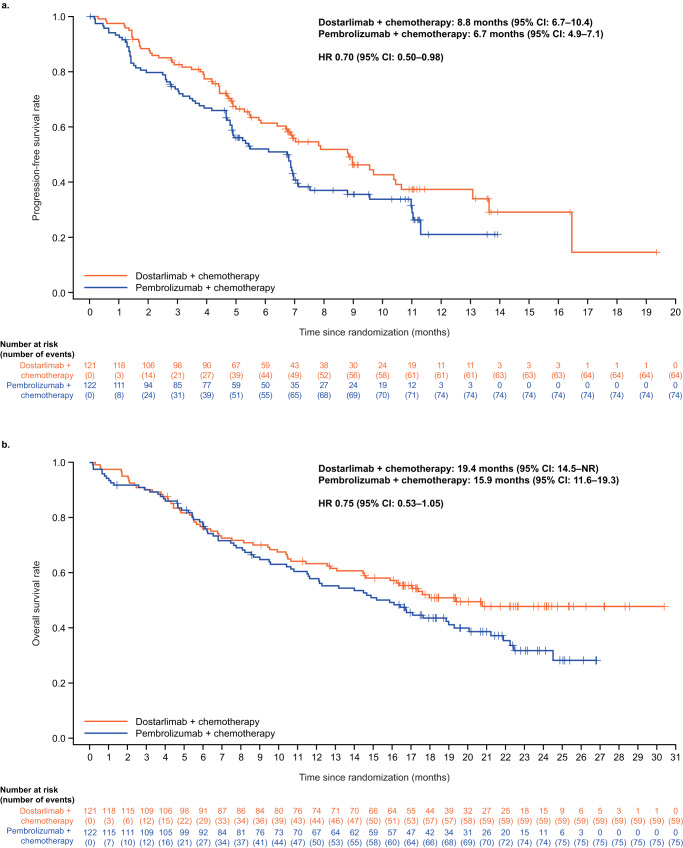
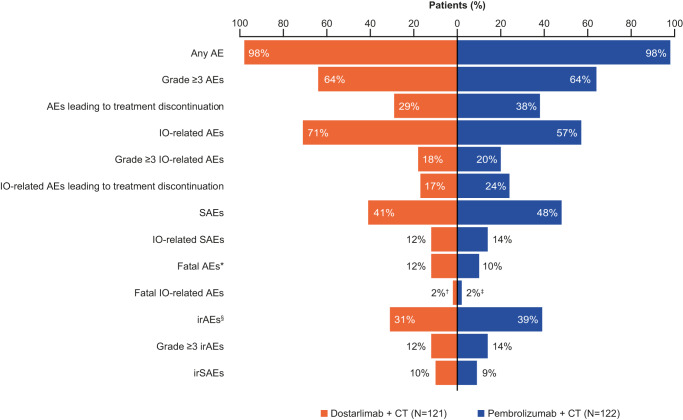
PERLA is a global, double-blind, parallel phase II trial (NCT04581824) comparing efficacy and safety of anti-PD-1 antibodies dostarlimab and pembrolizumab, plus chemotherapy (DCT and PCT, respectively) as first-line treatment in patients with metastatic non-squamous NSCLC without known targetable genomic aberrations. Patients stratified by PD-L1 tumor proportion score and smoking status were randomized 1:1, receiving ≤35 cycles 500 mg dostarlimab or 200 mg pembrolizumab, ≤35 cycles 500 mg/m2 pemetrexed and ≤4 cycles cisplatin (75 mg/m2) or carboplatin (AUC 5 mg/ml/min) Q3W. Primary endpoint was overall response rate (ORR) (blinded independent central review). Secondary endpoints include progression-free survival (PFS) based on investigator assessment, overall survival (OS) and safety. Exploratory endpoints include ORR by PD-L1 subgroup and duration of response. PERLA met its pre-specified endpoint. ORR (n/N; 95% CI) is 45% (55/121; 36.4-54.8) for DCT and 39% (48/122; 30.6-48.6) for PCT (data cut-off: 07 July 23), numerically favoring dostarlimab in PD-L1-positive subgroups. Median PFS (months [95% CI]) is 8.8 (6.7-10.4) for DCT and 6.7 (4.9-7.1) for PCT (HR 0.70 [95% CI: 0.50-0.98]; data cut-off: 04 August 22). Median OS (months [95% CI]) is 19.4 (14.5-NR) for DCT and 15.9 (11.6-19.3) for PCT (HR 0.75 [95% CI: 0.53-1.05]) (data cut-off: 07 July 23). Safety profiles are similar between groups. In this study, DCT shows similar efficacy to PCT and demonstrates clinical efficacy as first-line treatment for patients with metastatic non-squamous NSCLC.
© 2023. The Author(s).
Conflict of interest statement
S.M.L. has received research grants from Yuhan and Janssen; received consulting fees from AstraZeneca, Boehringer Ingelheim, Lilly, Takeda, Guardant and J Ints Bio; and received research grants from AstraZeneca, Beigene, Boehringer Ingelheim, GSK, Roche, Hengrui, BridgeBio Therapeutics, Oscotec, and Daichii-Sankyo. S.P. has an advisory role with AbbVie, AiCME, Amgen, Arcus, AstraZeneca, Bayer, Beigene, Biocartis, BioInvent, Blueprint Medicines, Boehringer Ingelheim, Bristol-Myers Squibb, Clovis, Daiichi Sankyo, Debiopharm, ecancer, Eli Lilly, Elsevier, F-Star, Fishawack, Foundation Medicine, Genzyme, Gilead, GSK, Illumina, Imedex, IQVIA, Incyte, iTeos, Janssen, Medscape, Medtoday, Merck Sharp and Dohme, Merck Serono, Merrimack, Novartis, Novocure, OncologyEducation, Pharma Mar, Phosplatin Therapeutics, PER, Peerview, Pfizer, PRIME, Regeneron, RMEI, Roche/Genentech, RTP, Sanofi, Seattle Genetics, Takeda, and Vaccibody; has been an invited speaker for AiCME, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, ecancer, Eli Lilly, Foundation Medicine, Illumina, Imedex, Medscape, Merck Sharp and Dohme, Mirati, Novartis, PER, Peerview, Pfizer, Prime, Roche/Genentech, RTP, Sanofi, and Takeda; and received research grants from Amgen, AstraZeneca, Beigene, Bristol-Myers Squibb, GSK, Merck Sharp and Dohme, and Roche/Genentech. A.L.O.G. is an employee of the Servicio Andaluz de Salud and has had an advisory role for Roche, Bristol Myers Squibb, and Merck Sharp Dohme. GdJP has no conflicts of interest to disclose. C.S.F. has been an invited speaker for Fundacion Respirar. G.L.R. has received consulting fees from Roche, Novartis, BMS, MSD, AstraZeneca, Takeda, Amgen, Sanofi, Italfarmaco and Pfizer; received honoraria from Roche, Novartis, BMS, MSD, AstraZeneca, Takeda, Amgen, and Sanofi; received travel grants from Roche, BMS, and MSD; had an advisory role for Roche, Novartis, BMS, MSD, AstraZeneca, and Sanofi; and been an investigator for clinical trials sponsored by Roche, Novartis, BMS, MSD, AstraZeneca, GSK, Amgen, and Sanofi. MS has had contracts for clinical trial activities (institutional and personal as site Principal Investigator) with GSK, Merck Serono, BMS, MSD, Roche, Sanofi, Regeneron, Astellas, Amgen, Bayer, BeiGene, Clovis, Tesaro, Gilead, Bioven, Novartis, Pfizer, Eli Lilly, Pharma Mar, AbbVie, Astra Zeneca, Mylan, and Daiichi Sankyo. JSA has been an invited speaker for Kyowa Kirin, Amgen Korea, Yuhan, AstraZeneca Korea, Menarini Korea, Bayer Korea, Takeda Phar, Novartis Korea, Hanmi, BC World, Pfizer, Roche Korea, and Boehringer Ingelheim; and had an advisory role for Yuhan, Bayer Korea, Yooyoung, Pharmbio Korea, Vifor Pharma, and Bixink. MR has had an advisory role for Amgen, AstraZeneca, Beigene, BMS, Boehringer Ingelheim, Daiichi-Sankyo, GSK, Lilly, Merck, MSD, Novartis, Pfizer, Regeneron, Roche, Samsun Bioepsis, and Sanofi. Z.S. is an employee of GSK. N.H. is a former employee of GSK (at time of study) and is a current employee of Lantheus Medical Imaging. E.Z. is an employee of GSK. E.B. is an employee of GSK and holds stocks/shares in GSK. N.S. is an employee of GSK and their spouse works for Debiopharm. S.O’.D. is an employee of GSK and their spouse works as a federal employee. F.d.M. has had an advisory role for AstraZeneca, Roche, Novartis, Merck, BMS, and MSD.
Figures
References
-
- GLOBOCAN. Lung cancer factsheet. https://gco.iarc.fr/today/data/factsheets/cancers/15-Lung-fact-sheet.pdf (2020).
-
- American Cancer Society. Cancer Facts and Figures. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-... (2022).
-
- Planchard, D. et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up (update available at https://www.esmo.org/content/download/347819/6934778/1/ESMO-CPG-mNSCLC-1...) (accessed November 2022). Ann. Oncol. 29Suppl4, iv192-iv237 (2018). - PubMed
-
- Cancer.net. Lung cancer non-small cell: statistics. https://www.cancer.net/cancer-types/lung-cancer-non-small-cell/statistics (2022).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
