

Bag-Valve-Mask Ventilation and Survival From Out-of-Hospital Cardiac Arrest: A Multicenter Study
- PMID: 37952192
- PMCID: PMC10840971
- DOI: 10.1161/CIRCULATIONAHA.123.065561
Bag-Valve-Mask Ventilation and Survival From Out-of-Hospital Cardiac Arrest: A Multicenter Study
Abstract
Background: Few studies have measured ventilation during early cardiopulmonary resuscitation (CPR) before advanced airway placement. Resuscitation guidelines recommend pauses after every 30 chest compressions to deliver ventilations. The effectiveness of bag-valve-mask ventilation delivered during the pause in chest compressions is unknown. We sought to determine: (1) the incidence of lung inflation with bag-valve-mask ventilation during 30:2 CPR; and (2) the association of ventilation with outcomes after out-of-hospital cardiac arrest.
Methods: We studied patients with out-of-hospital cardiac arrest from 6 sites of the Resuscitation Outcomes Consortium CCC study (Trial of Continuous Compressions versus Standard CPR in Patients with Out-of-Hospital Cardiac Arrest). We analyzed patients assigned to the 30:2 CPR arm with ≥2 minutes of thoracic bioimpedance signal recorded with a cardiac defibrillator/monitor. Detectable ventilation waveforms were defined as having a bioimpedance amplitude ≥0.5 Ω (corresponding to ≥250 mL VT) and a duration ≥1 s. We defined a chest compression pause as a 3- to 15-s break in chest compressions. We compared the incidence of ventilation and outcomes in 2 groups: patients with ventilation waveforms in <50% of pauses (group 1) versus those with waveforms in ≥50% of pauses (group 2).
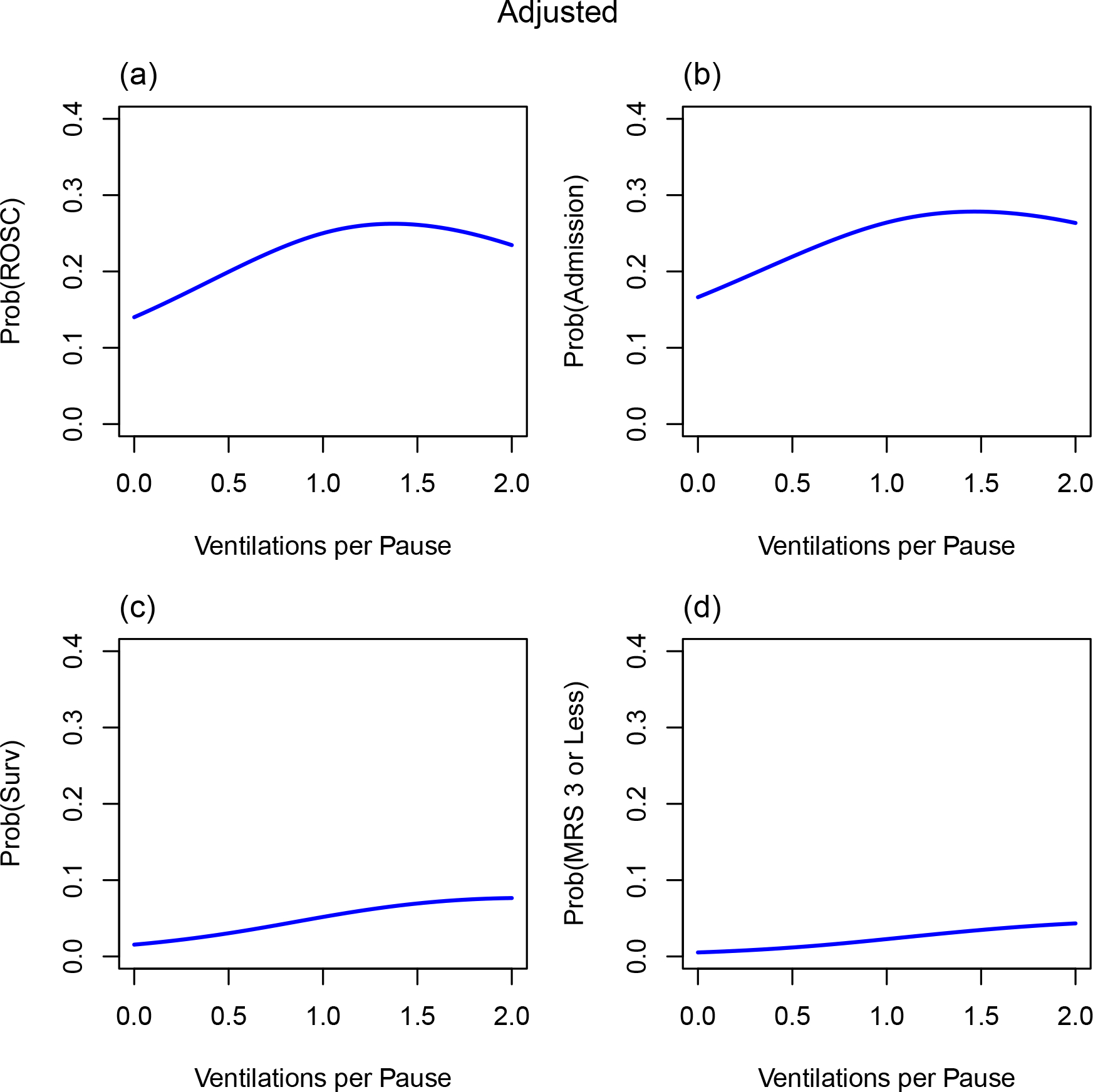
Results: Among 1976 patients, the mean age was 65 years; 66% were male. From the start of chest compressions until advanced airway placement, mean±SD duration of 30:2 CPR was 9.8±4.9 minutes. During this period, we identified 26 861 pauses in chest compressions; 60% of patients had ventilation waveforms in <50% of pauses (group 1, n=1177), and 40% had waveforms in ≥50% of pauses (group 2, n=799). Group 1 had a median of 12 pauses and 2 ventilations per patient versus group 2, which had 12 pauses and 12 ventilations per patient. Group 2 had higher rates of prehospital return of spontaneous circulation (40.7% versus 25.2%; P<0.0001), survival to hospital discharge (13.5% versus 4.1%; P<0.0001), and survival with favorable neurological outcome (10.6% versus 2.4%; P<0.0001). These associations persisted after adjustment for confounders.
Conclusions: In this study, lung inflation occurred infrequently with bag-valve-mask ventilation during 30:2 CPR. Lung inflation in ≥50% of pauses was associated with improved return of spontaneous circulation, survival, and survival with favorable neurological outcome.
Keywords: cardiography, impedance; cardiopulmonary resuscitation; heart arrest; patient outcome assessment; ventilation.
Conflict of interest statement
Figures


Comment in
-
"Hard and Fast" Resuscitation Guidelines May Need a Bit of "Breathing" Room.Circulation. 2023 Dec 5;148(23):1857-1859. doi: 10.1161/CIRCULATIONAHA.123.066071. Epub 2023 Nov 12. Circulation. 2023. PMID: 37952160 No abstract available.
References
-
- Tsao CW, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, Baker-Smith CM, Beaton AZ, Boehme AK, Buxton AE, Commodore-Mensah Y, Elkind MSV, Evenson KR, Eze-Nliam C, Fugar S, Generoso G, Heard DG, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation. 2023;147:e93–e621. doi: 10.1161/CIR.0000000000001123. - DOI - PMC - PubMed
-
- Taniguchi D, Baernstein A, Nichol G. Cardiac Arrest: A Public Health Perspective. Emerg Med Clin North Am. 2012;30:1–12. - PubMed
-
- Idris AH, Guffey D, Pepe PE, Brown SP, Brooks SC, Callaway CW, Christenson J, Davis DP, Daya MR, Gray R, et al. ; Resuscitation Outcomes Consortium Investigators. Chest compression rates and survival following out-of-hospital cardiac arrest. Crit Care Med. 2015;43:840–8.. - PubMed
-
- Stiell IG, Brown SP, Nichol G, Cheskes S, Vaillancourt C, Callaway CW, Morrison LJ, Christenson J, Aufderheide TP, Davis DP, et al. What Is the Optimal Chest Compression Depth During Out-of-Hospital Cardiac Arrest Resuscitation of Adult Patients? Circulation. 2014;130:1962–1970. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
