

Inflammatory dilated cardiomyopathy associated with psoriasis: a case report
- PMID: 37953296
- PMCID: PMC10641966
- DOI: 10.1186/s13256-023-04207-2
Inflammatory dilated cardiomyopathy associated with psoriasis: a case report
Abstract
Background: Psoriasis is a chronic inflammatory skin disease with a genetic basis. Psoriasis is accepted as a systemic, immune-mediated disease. Hypertension, obesity, metabolic disorders including diabetes mellitus and hyperlipidemia, and psychiatric disorders are more prevalent among children with psoriasis compared to children without psoriasis. In this study, we report a case of dramatic response of inflammatory cardiomyopathy to anti-inflammatory treatment of psoriasis; which might reveal similar pathogenesis basis of these two diseases.
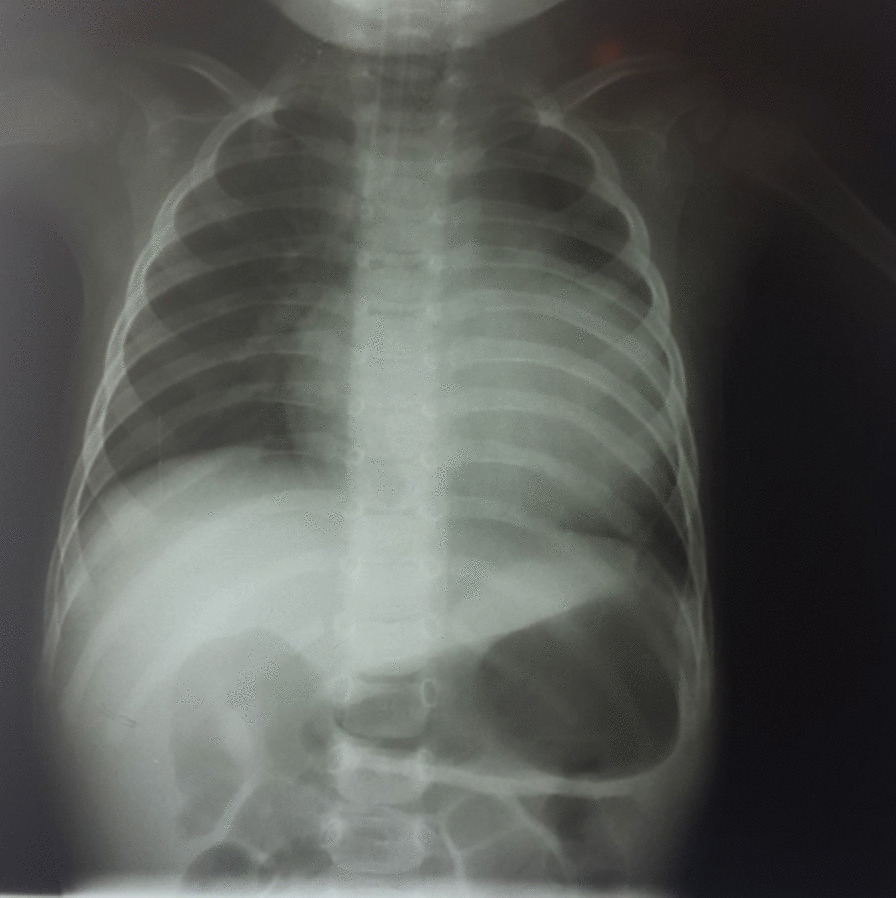
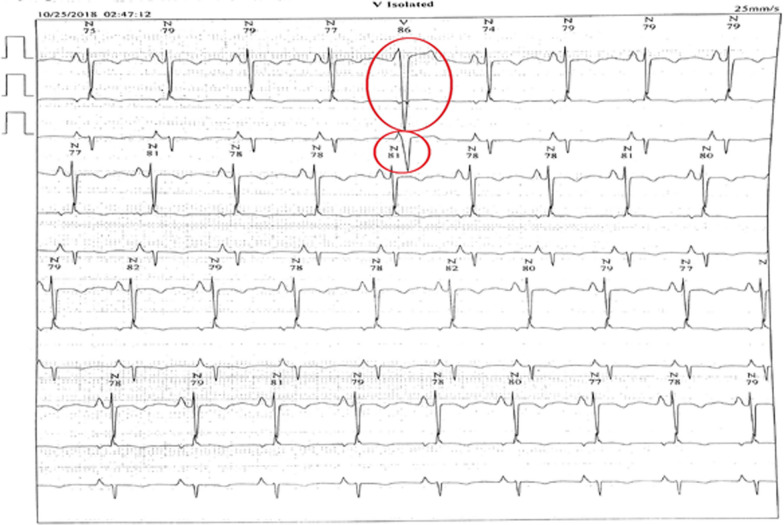
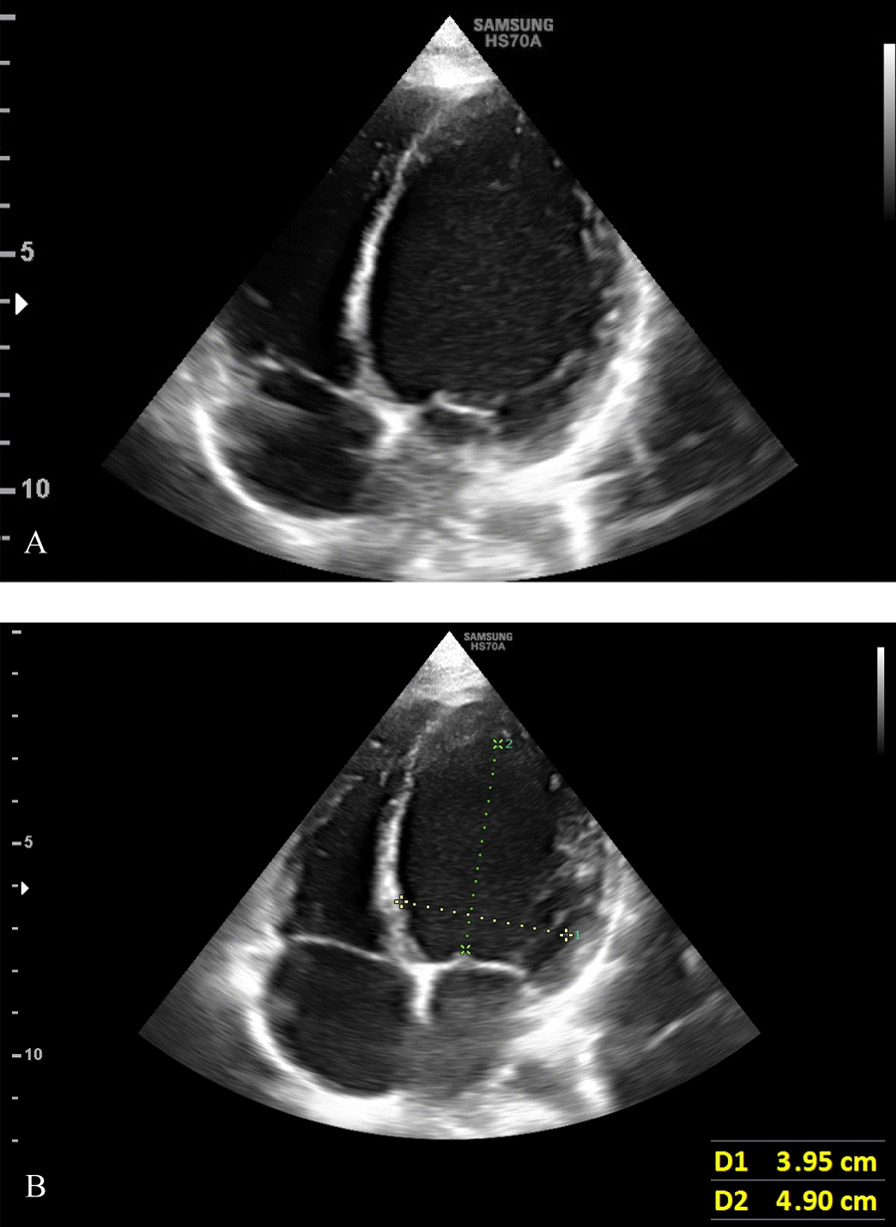
Case presentation: A 9-year-old Caucasian boy presenting with signs and symptoms of heart failure refractory to conventional therapies was admitted to our pediatric cardiology service. As the patient also had psoriasis, and considering the fact that there might be an association between the two conditions, immunosuppressive drugs were administered, which led to a dramatic improvement in heart function.
Conclusions: The results of this study add to evidence linking psoriasis with inflammatory dilated cardiomyopathy. Clinicians, particularly cardiologists, must pay special attention to the cardiac complications of systemic diseases.
Keywords: Case report; Heart failure; Inflammatory cardiomyopathy; Psoriasis.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors have no competing interests.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
