

Vascular tumors of the liver: A brief review
- PMID: 37953709
- PMCID: PMC10700950
- DOI: 10.14701/ahbps.23-046
Vascular tumors of the liver: A brief review
Abstract
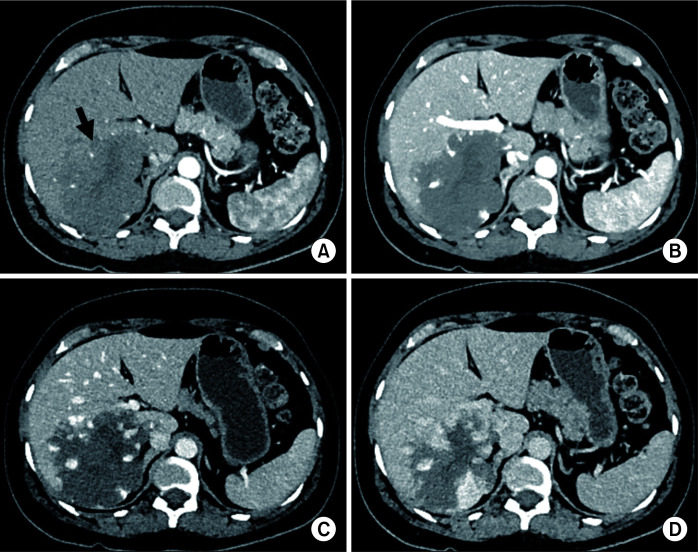
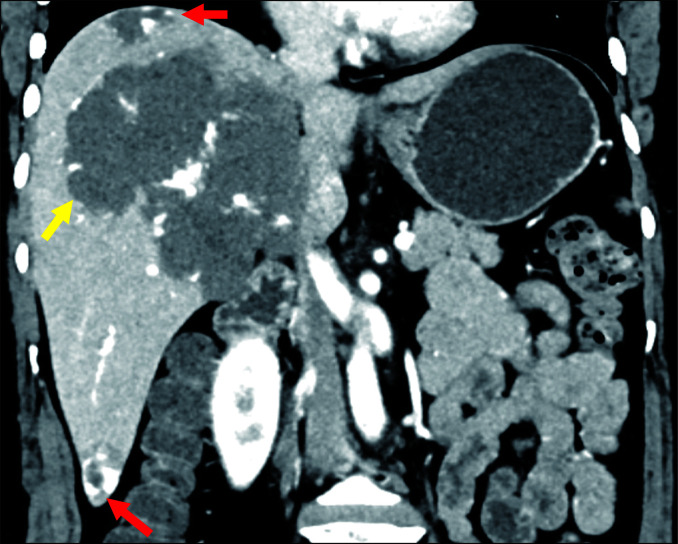
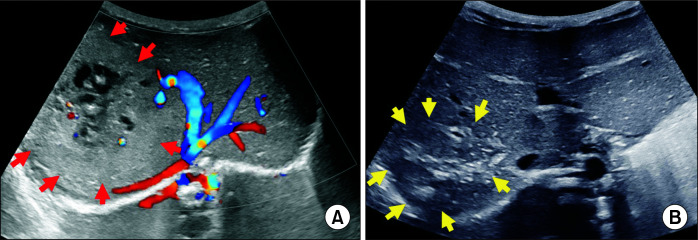
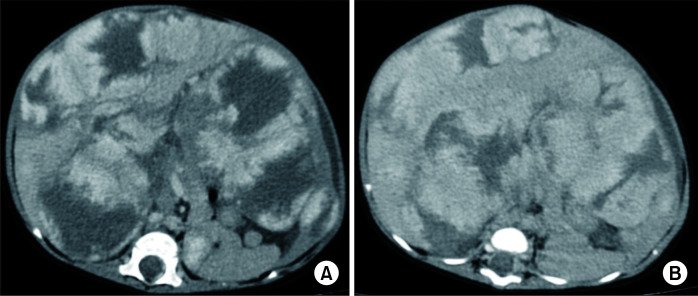
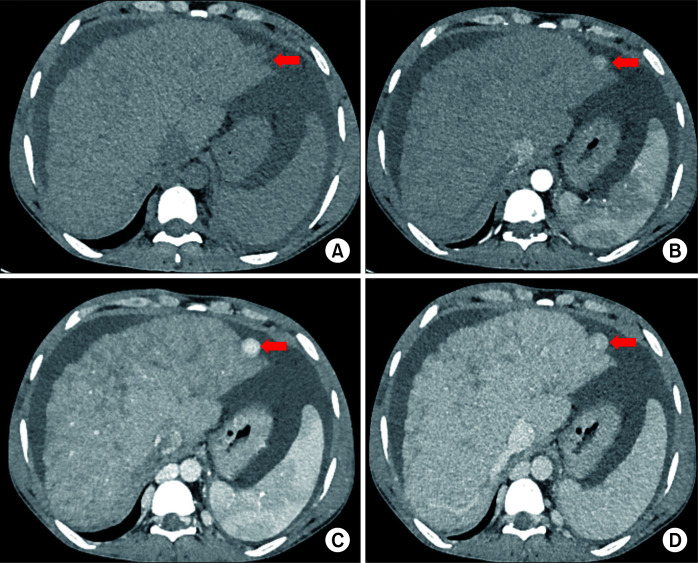
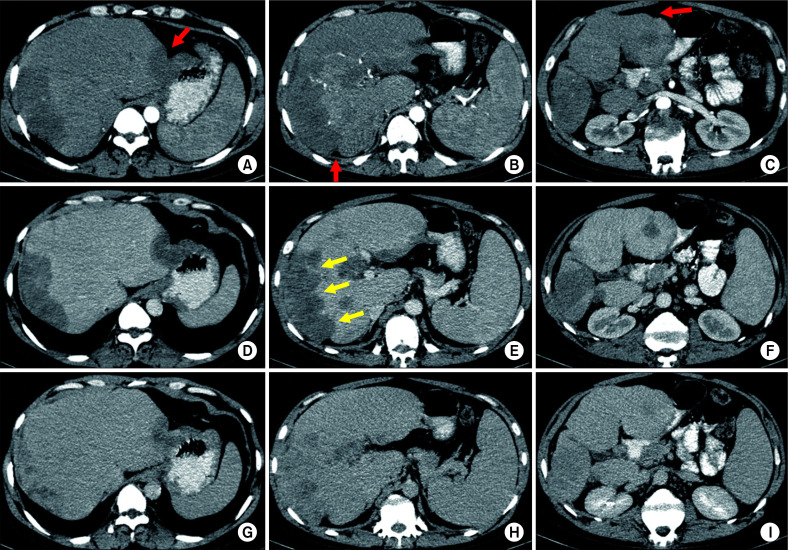
Vascular tumors of the liver are mesenchymal lesions from endothelial cells. They range from common benign lesions such as haemangioma, intermediate tumors like Kaposi sarcoma, and perivascular epithelioid cell tumor to malignant tumors such as hepatic epithelioid hemangioendothelioma and hepatic angiosarcoma in adults. Pediatric vascular tumors of the liver also include benign, locally aggressive, borderline, and malignant masses with haemangiomas being the most common benign tumors and epithelioid hemangioendothelioma being an uncommon pediatric malignancy. The list of these lesions is completed by nodular regenerative hyperplasia, solitary fibrous tumour, and hepatic small vessel neoplasms (HSVN). Some of these tumors are uncommon and rare. This review article aimed to enumerate hepatic vascular tumors along with their imaging, histopathology, molecular findings for accurate diagnosis that can result in better management.
Keywords: Diagnostic; Liver; Vascular tumour.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- WHO Classification of Tumours Editorial Board, author. Soft tissue and bone tumours. 5th ed. Vol 3. International Agency for Research on Cancer; 2020.
Publication types
LinkOut - more resources
Full Text Sources