

Uterocolon Fistula Formation in 50 Year Old Patient with History of 16 Years Intrauterine Device Use: A Case Report
- PMID: 37954089
- PMCID: PMC10637201
- DOI: 10.2147/IMCRJ.S425424
Uterocolon Fistula Formation in 50 Year Old Patient with History of 16 Years Intrauterine Device Use: A Case Report
Abstract
Introduction: Uterocolon fistula is one of the complications of intrauterine device (IUD) insertion. Not only may IUD materials cause perforation, but some other risk factors may contribute to its development including uterine abnormalities, thus IUD is contraindicated in patients with anatomical anomaly.
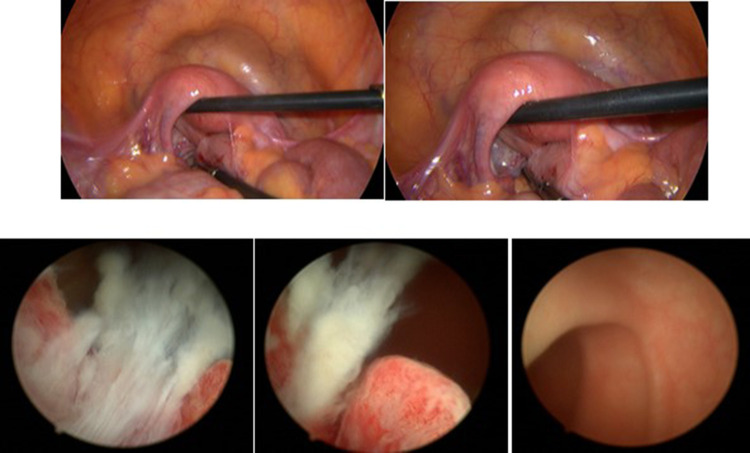
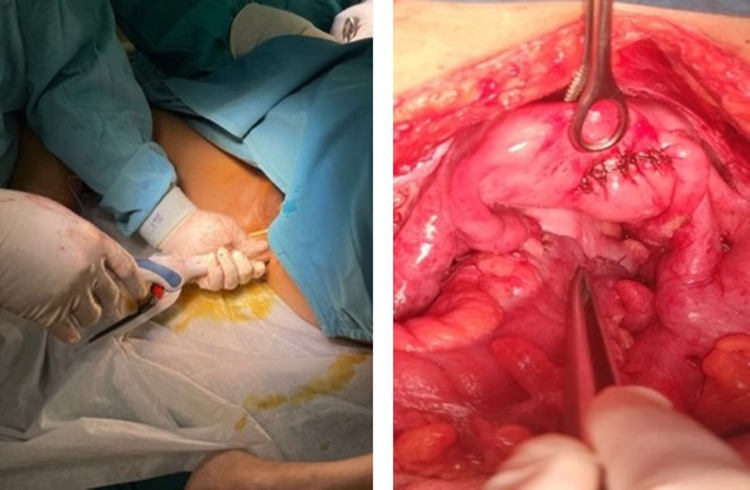
Case: P3A1 woman, 50 years old with a history of IUD use for 16 years presented with complaints of fecal discharge from the vagina 8 months ago which worsened after IUD extraction. Physical examination revealed no abdominal tenderness. Speculum examination found feces in the cervical canal. CT scan examination showed multiple uterocolon fistulas and uterine didelphys. Diagnostic laparoscopy and hysteroscopy were carried out and found a recto-uterine fistula, then the patient was scheduled for colostomy and reanastomosis with the stapler method.
Conclusion: Diagnosis was very difficult to establish despite proper imaging modalities. The use of direct visual diagnostics (hysteroscopy and laparoscopy) can be a good alternative for the diagnosis of uterocolon fistula. To the best of our knowledge, this is the first case report on recto-uterine fistula in a patient with long-term use of IUD and uterine didelphys.
Keywords: IUD; diagnostics; uterine didelphys; uterocolon fistula.
© 2023 Gurnita and Achmad.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures

Similar articles
-
Complete and partial uterine perforation and embedding following insertion of intrauterine devices. II. Diagnostic methods, prevention, and management.Obstet Gynecol Surv. 1981 Aug;36(8):401-17. doi: 10.1097/00006254-198108000-00001. Obstet Gynecol Surv. 1981. PMID: 6455610 Review.
-
Colocolic fistula caused by a previously inserted intrauterine device. Case report.Contraception. 1997 Nov;56(5):337-9. doi: 10.1016/s0010-7824(97)00161-3. Contraception. 1997. PMID: 9437564
-
Asymptomatic cecal perforation and ileocecal fistula after intrauterine device migration: a case report.J Surg Case Rep. 2020 Apr 3;2020(4):rjaa015. doi: 10.1093/jscr/rjaa015. eCollection 2020 Apr. J Surg Case Rep. 2020. PMID: 32269751 Free PMC article.
-
Migrated intrauterine device: Case series report.Int J Surg Case Rep. 2023 Oct;111:108631. doi: 10.1016/j.ijscr.2023.108631. Epub 2023 Aug 11. Int J Surg Case Rep. 2023. PMID: 37757734 Free PMC article.
-
Ileal penetration by a Multiload-Cu 375 intrauterine contraceptive device. A case report with review of the literature.Contraception. 1998 Nov;58(5):295-304. doi: 10.1016/s0010-7824(98)00116-4. Contraception. 1998. PMID: 9883385 Review.
Cited by
-
A utero-pelvic fistula and pelvic-parasitic myoma by hysteroscopic resection of a recurrent submucosal myoma: a case report.Front Med (Lausanne). 2025 Jun 20;12:1579105. doi: 10.3389/fmed.2025.1579105. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40620430 Free PMC article.
References
-
- Amies Oelschlager A-M, Debiec K, Micks E, Prager S. Use of the levonorgestrel intrauterine system in adolescents with known uterine didelphys or unicornuate uterus. J Pediatr Adolesc Gynecol. 2013;26(2):e58. doi:10.1016/j.jpag.2013.01.029 - DOI
-
- Espey E, Ogburn T, Hall R, Byrn F. Use of intrauterine device in the setting of uterus didelphys. Obstet Gynecol. 2006;108(3):774–776. doi:10.1097/01.AOG.0000198633.77911.de - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
