

Metabolic dysfunction-associated steatotic liver disease increases the risk of incident cardiovascular disease: a nationwide cohort study
- PMID: 37954905
- PMCID: PMC10632413
- DOI: 10.1016/j.eclinm.2023.102292
Metabolic dysfunction-associated steatotic liver disease increases the risk of incident cardiovascular disease: a nationwide cohort study
Abstract
Background: The various subcategories under the overarching term of steatotic liver disease (SLD) have been recently proposed by the nomenclature consensus group and endorsed by international academic liver societies. Our aim was to investigate the association between each subtype of SLD and incident cardiovascular disease (CVD) in a nationwide Korean cohort.
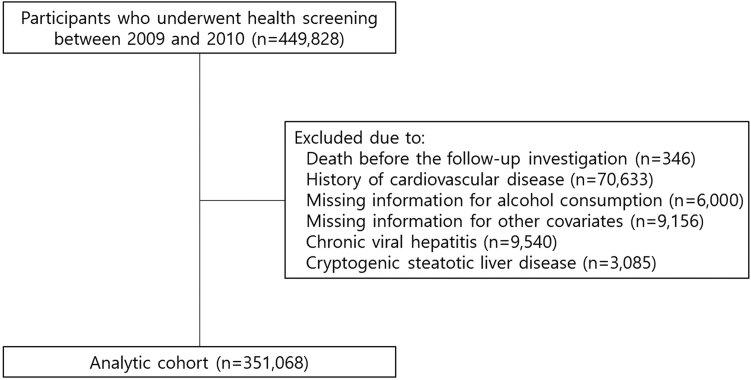
Methods: From a nationwide health screening database from Korea, 351,068 individuals aged 47-86 years between January 1, 2009 and December 31, 2010 were included and followed until December 31, 2019 for a median of 9.0 years. Individuals were categorised into no SLD, metabolic dysfunction-associated steatotic liver disease (MASLD), MASLD with increased alcohol intake (MetALD), and alcohol-related liver disease (ALD). Hepatic steatosis was defined as fatty liver index ≥60. The primary outcome was a composite CVD, which includes non-fatal and fatal myocardial infarction and stroke. The subdistribution hazard ratio (SHR) was calculated using the Fine-Gray model with treating non-CVD-related death as a competing risk.
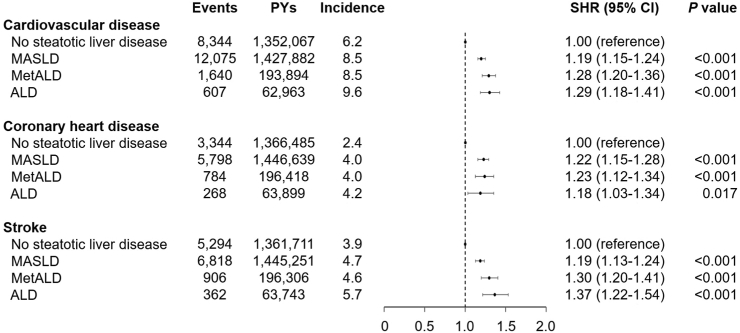
Findings: There were 199,817 male (56.9%) and 151,251 female (43.1%) with a median age of 55 years (interquartile range, 50-61). The prevalence of no SLD, MASLD, MetALD, and ALD was 44.3%, 47.2%, 6.4%, and 2.1%, respectively; and the incidence rate of CVD in each subcategory was 6.2, 8.5, 8.5, and 9.6 per 1000 person-years, respectively. MASLD (SHR, 1.19; 95% confidence interval [CI], 1.15-1.24), MetALD (SHR, 1.28; 95% CI, 1.20-1.36), and ALD (SHR, 1.29; 95% CI, 1.18-1.41) increased the risk of CVD compared to no SLD, which increment was in consecutive order (Ptrend < 0.001).
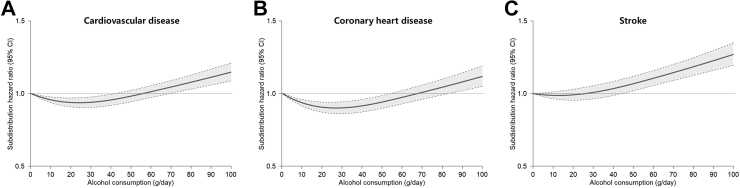
Interpretation: Individuals with MASLD, MetALD, or ALD are at an increased risk of developing incident CVD. Higher risk of CVD observed in MetALD compared to MASLD suggests the additive impact of alcohol consumption in conjunction with cardiometabolic risk factors on CVD development. These findings support and validate the utility of the new consensus criteria for SLD in predicting CVD.
Funding: The National Research Foundation of Korea and the Korea Centers for Disease Control and Prevention.
Keywords: Cardiovascular disease; Cardiovascular risk factors; Metabolic dysfunction-associated steatotic liver disease; Nonalcoholic fatty liver disease.
© 2023 The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Eslam M., Newsome P.N., Sarin S.K., et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73(1):202–209. - PubMed
-
- Targher G., Byrne C.D., Lonardo A., Zoppini G., Barbui C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: a meta-analysis. J Hepatol. 2016;65(3):589–600. - PubMed
-
- Mantovani A., Csermely A., Petracca G., et al. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: an updated systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(11):903–913. - PubMed
LinkOut - more resources
Full Text Sources
