Tisagenlecleucel utilisation and outcomes across refractory, first relapse and multiply relapsed B-cell acute lymphoblastic leukemia: a retrospective analysis of real-world patterns
- PMID: 37954907
- PMCID: PMC10632672
- DOI: 10.1016/j.eclinm.2023.102268
Tisagenlecleucel utilisation and outcomes across refractory, first relapse and multiply relapsed B-cell acute lymphoblastic leukemia: a retrospective analysis of real-world patterns
Abstract
Background: Tisagenlecleucel was approved by the Food and Drug Administration (FDA) in 2017 for refractory B-cell acute lymphoblastic leukemia (B-ALL) and B-ALL in ≥2nd relapse. Outcomes of patients receiving commercial tisagenlecleucel upon 1st relapse have yet to be established. We aimed to report real-world tisagenlecleucel utilisation patterns and outcomes across indications, specifically including patients treated in 1st relapse, an indication omitted from formal FDA approval.
Methods: We conducted a retrospective analysis of real-world tisagenlecleucel utilisation patterns across 185 children and young adults treated between August 30, 2017 and March 6, 2020 from centres participating in the Pediatric Real-World CAR Consortium (PRWCC), within the United States. We described definitions of refractory B-ALL used in the real-world setting and categorised patients by reported Chimeric Antigen Receptor (CAR) T-cell indication, including refractory, 1st relapse and ≥2nd relapse B-ALL. We analysed baseline patient characteristics and post-tisagenlecleucel outcomes across defined cohorts.
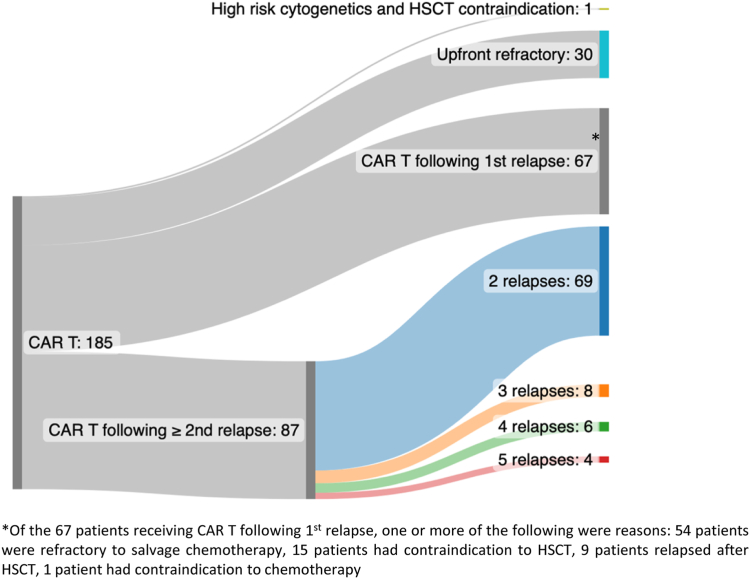
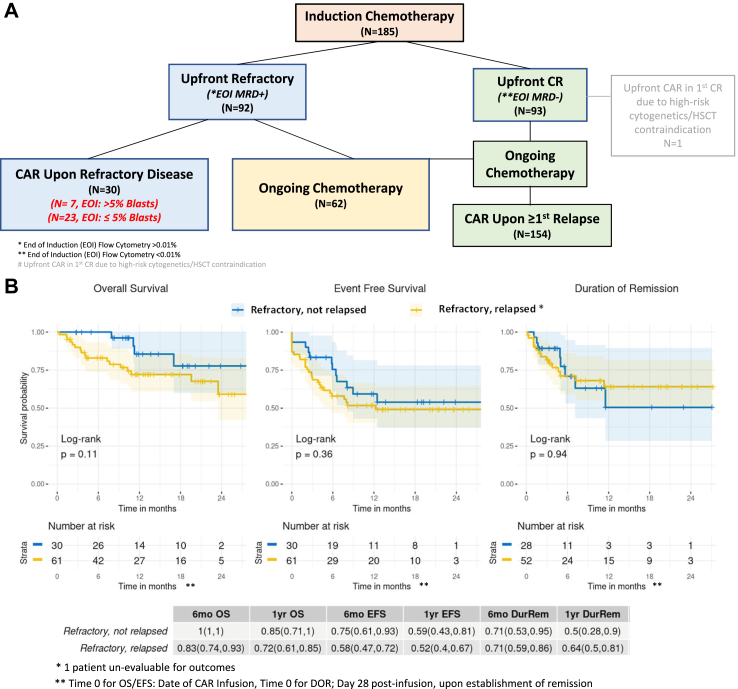
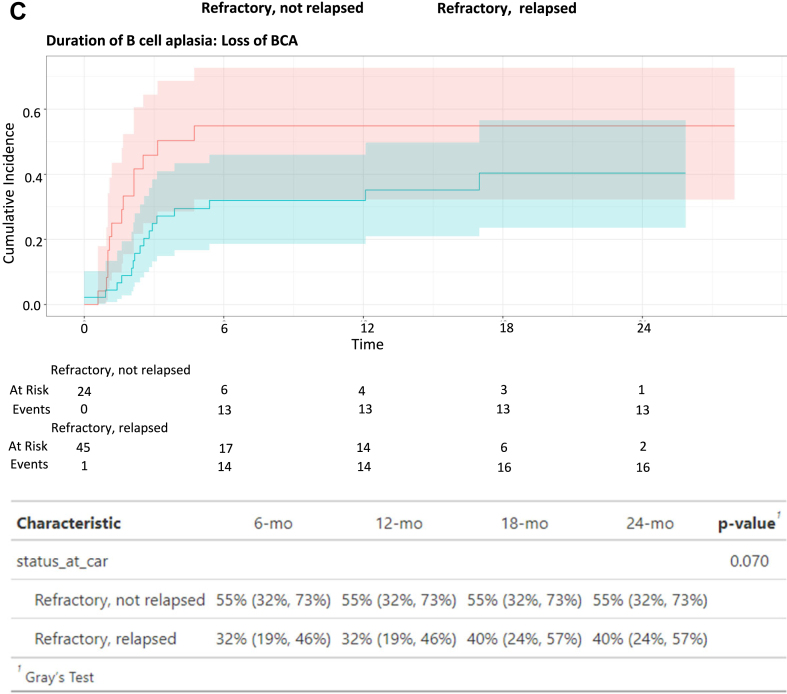
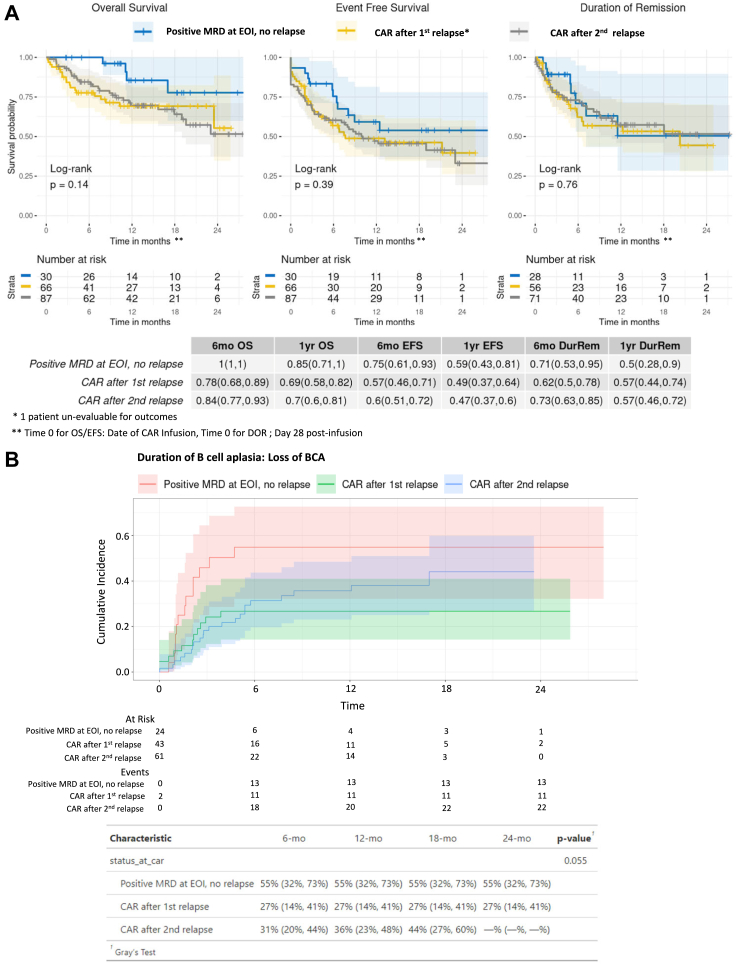
Findings: Thirty-six percent (n = 67) of our cohort received tisagenlecleucel following 1st relapse. Of 66 evaluable patients, 56 (85%, 95% CI 74-92%) achieved morphologic complete response. Overall-survival (OS) and event-free survival (EFS) at 1-year were 69%, (95% CI 58-82%) and 49%, (95% CI 37-64%), respectively, with survival outcomes statistically comparable to remaining patients (OS; p = 0.14, EFS; p = 0.39). Notably, toxicity was increased in this cohort, warranting further study. Interestingly, of 30 patients treated for upfront refractory disease, 23 (77%, 95% CI 58-90%) had flow cytometry and/or next-generation sequencing (NGS) minimum residual disease (MRD)-only disease at the end of induction, not meeting the historic morphologic definition of refractory.
Interpretation: Our findings suggested that tisagenlecleucel response and survival rates overlap across patients treated with upfront refractory B-ALL, B-ALL ≥2nd relapse and B-ALL in 1st relapse. We additionally highlighted that definitions of refractory B-ALL are evolving beyond morphologic measures of residual disease.
Funding: St. Baldrick's/Stand Up 2 Cancer, Parker Institute for Cancer Immunotherapy, Virginia and D.K. Ludwig Fund for Cancer Research.
Keywords: CAR T cells; CD19 CAR T cells; Commercial CAR; First relapse; Immunotherapy; Pediatric oncology; Real-world analysis; Tisagenlecleucel.
© 2023 The Authors.
Conflict of interest statement
V.B. serves on the boards of ArsenalBio and Umoja Biopharma and consults or holds stock in Zafrens and Treeline Biosciences which are developing therapies for cancer treatment and Illumina, Invitae, Pacific Biosciences, and Guardant who are developing oncology NGS tests. C.L.M. is an inventor on several patents related to CAR T-cell therapies. C.L.M. is a cofounder of Lyell Immunopharma, CARGO Therapeutics and Link Cell Therapies, which are developing CAR-based therapies, and consults for Lyell, CARGO, Link, Ensoma, Mammoth, Immatics, Apricity, Glaxo Smith Klein, Nektar, Legend and Bristol Myers Squibb. C.L.M receives royalties for CD-22 CAR licensing from NIH, has had grant/contract funding from St. Baldrick’s Foundation, NIH, CIRM, Parker, Tune therapeutics, Lyell Immunopharma, Ludwig Institute, Emerson Collective, Department of Defense and Goldhirsh-Yellin Foundation. She is a member of the Board of Directors of CARGO Therapeutics and Link Cell Therapies and owns stocks in Lyell Immunopharma, CARGO Therapeutics, Link Cell Therapies, Ensoma, Mammoth and Apricity. T.W.L. served on advisory boards or consults for Novartis, Bayer, Aptitude Health, Jumo Health, Massive Bio, Medscape, AI Therapeutics, Jazz Pharmaceuticals, GentiBio, Menarini, Pyramid Biosciences, Targeted Oncology, Treeline Biosciences. He owns stocks/other ownership interest in advanced microbubbles. T.W.L. received research funding from Lily, Roche/Genentech, Taiho Oncology, Advanced Accelerator Applications/Novartis, Bristol-Myers Squibb, BioAtla, Pfizer, Bayer and Turning Point Therapeutics. G.D.M. received funding for medical writing from Novartis. C.L.P. served on an advisory board for Novartis. L.S. served on an advisory board for Novartis. H.S. served on an advisory board for Novartis. M.H. served on editorial advisory board for Novartis and Sobi Pharmaceuticals and is the Vice Chair for COG NHL committee and COG NHL Biology Committee. V.F. consulted for Adaptimmune. S.P. is supported by the UCSF-Stanford CERSI grant UOI FD005978 from the FDA. P.S. served on advisory board for Sobi Pharmaceuticals. A.K. received COG support for meeting attendance. K.J.C. received grant support for an investigator-initiated trial and sat on advisory boards for Novartis and Atara Biotherapeutics. M.R.V. consults for Novartis, Sanofi, Qihan, Forge, Takada and Equillium. M.R.V. has a provisional patent describing methods of producing and using immunotherapy for cancer. M.R.V.participates on the safety monitoring/advisory board for FBX-101 and owns stocks/options for Fate therapeutics.
Figures