

Torsemide vs Furosemide Among Patients With New-Onset vs Worsening Chronic Heart Failure: A Substudy of the TRANSFORM-HF Randomized Clinical Trial
- PMID: 37955908
- PMCID: PMC10644243
- DOI: 10.1001/jamacardio.2023.4776
Torsemide vs Furosemide Among Patients With New-Onset vs Worsening Chronic Heart Failure: A Substudy of the TRANSFORM-HF Randomized Clinical Trial
Abstract
Importance: Differences in clinical profiles, outcomes, and diuretic treatment effects may exist between patients with de novo heart failure (HF) and worsening chronic HF (WHF).
Objectives: To compare clinical characteristics and treatment outcomes of torsemide vs furosemide in patients hospitalized with de novo HF vs WHF.
Design, setting, and participants: All patients with a documented ejection fraction who were randomized in the Torsemide Comparison With Furosemide for Management of Heart Failure (TRANSFORM-HF) trial, conducted from June 18 through March 2022, were included in this post hoc analysis. Study data were analyzed March to May 2023.
Exposure: Patients were categorized by HF type and further divided by loop diuretic strategy.
Main outcomes and measures: End points included all-cause mortality and hospitalization outcomes over 12 months, as well as change from baseline in the Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS).
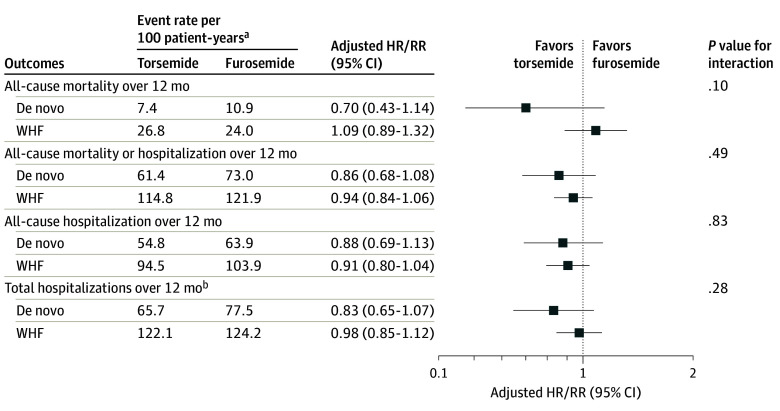
Results: Among 2858 patients (mean [SD] age, 64.5 [14.0] years; 1803 male [63.1%]), 838 patients (29.3%) had de novo HF, and 2020 patients (70.7%) had WHF. Patients with de novo HF were younger (mean [SD] age, 60.6 [14.5] years vs 66.1 [13.5] years), had a higher glomerular filtration rate (mean [SD], 68.6 [24.9] vs 57.0 [24.0]), lower levels of natriuretic peptides (median [IQR], brain-type natriuretic peptide, 855.0 [423.0-1555.0] pg/mL vs 1022.0 [500.0-1927.0] pg/mL), and tended to be discharged on lower doses of loop diuretic (mean [SD], 50.3 [46.2] mg vs 63.8 [52.4] mg). De novo HF was associated with lower all-cause mortality at 12 months (de novo, 65 of 838 [9.1%] vs WHF, 408 of 2020 [25.4%]; adjusted hazard ratio [aHR], 0.50; 95% CI, 0.38-0.66; P < .001). Similarly, lower all-cause first rehospitalization at 12 months and greater improvement from baseline in KCCQ-CSS at 12 months were noted among patients with de novo HF (median [IQR]: de novo, 29.94 [27.35-32.54] vs WHF, 23.68 [21.62-25.74]; adjusted estimated difference in means: 6.26; 95% CI, 3.72-8.81; P < .001). There was no significant difference in mortality with torsemide vs furosemide in either de novo (No. of events [rate per 100 patient-years]: torsemide, 27 [7.4%] vs furosemide, 38 [10.9%]; aHR, 0.70; 95% CI, 0.40-1.14; P = .15) or WHF (torsemide 212 [26.8%] vs furosemide, 196 [24.0%]; aHR, 1.08; 95% CI, 0.89-1.32; P = .42; P for interaction = .10), In addition, no significant differences in hospitalizations, first all-cause hospitalization, or total hospitalizations at 12 months were noted with a strategy of torsemide vs furosemide in either de novo HF or WHF.
Conclusions and relevance: Among patients discharged after hospitalization for HF, de novo HF was associated with better clinical and patient-reported outcomes when compared with WHF. Regardless of HF type, there was no significant difference between torsemide and furosemide with respect to 12-month clinical or patient-reported outcomes.
Conflict of interest statement
Figures
Similar articles
-
Effect of Torsemide Versus Furosemide on Symptoms and Quality of Life Among Patients Hospitalized for Heart Failure: The TRANSFORM-HF Randomized Clinical Trial.Circulation. 2023 Jul 11;148(2):124-134. doi: 10.1161/CIRCULATIONAHA.123.064842. Epub 2023 May 22. Circulation. 2023. PMID: 37212600 Free PMC article. Clinical Trial.
-
Effect of Torsemide vs Furosemide After Discharge on All-Cause Mortality in Patients Hospitalized With Heart Failure: The TRANSFORM-HF Randomized Clinical Trial.JAMA. 2023 Jan 17;329(3):214-223. doi: 10.1001/jama.2022.23924. JAMA. 2023. PMID: 36648467 Free PMC article. Clinical Trial.
-
On-treatment analysis of torsemide versus furosemide for patients hospitalized for heart failure: A post-hoc analysis of TRANSFORM-HF.Eur J Heart Fail. 2024 Jul;26(7):1518-1523. doi: 10.1002/ejhf.3293. Epub 2024 May 15. Eur J Heart Fail. 2024. PMID: 38745502 Free PMC article. Clinical Trial.
-
A comprehensive review of the loop diuretics: should furosemide be first line?Ann Pharmacother. 2009 Nov;43(11):1836-47. doi: 10.1345/aph.1M177. Epub 2009 Oct 20. Ann Pharmacother. 2009. PMID: 19843838 Review.
-
An evaluation of torsemide in patients with heart failure and renal disease.Expert Rev Cardiovasc Ther. 2022 Jan;20(1):5-11. doi: 10.1080/14779072.2022.2022474. Epub 2022 Jan 3. Expert Rev Cardiovasc Ther. 2022. PMID: 34936522 Free PMC article. Review.
Cited by
-
Diuretics: a review of the pharmacology and effects on glucose homeostasis.Front Pharmacol. 2025 Mar 28;16:1513125. doi: 10.3389/fphar.2025.1513125. eCollection 2025. Front Pharmacol. 2025. PMID: 40223924 Free PMC article. Review.
-
A disproportionality analysis of adverse events associated with loop diuretics in the FDA Adverse Event Reporting System (FAERS).BMC Pharmacol Toxicol. 2025 Mar 17;26(1):63. doi: 10.1186/s40360-025-00890-7. BMC Pharmacol Toxicol. 2025. PMID: 40098168 Free PMC article.
References
-
- Mebazaa A, Yilmaz MB, Levy P, et al. . Recommendations on pre-hospital and early hospital management of acute heart failure: a consensus paper from the Heart Failure Association of the European Society of Cardiology, the European Society of Emergency Medicine and the Society of Academic Emergency Medicine–short version. Eur Heart J. 2015;36(30):1958-1966. doi:10.1093/eurheartj/ehv066 - DOI - PubMed
-
- Mentz RJ, Anstrom KJ, Eisenstein EL, et al. ; TRANSFORM-HF Investigators . Effect of torsemide vs furosemide after discharge on all-cause mortality in patients hospitalized with heart failure: the TRANSFORM-HF randomized clinical trial. JAMA. 2023;329(3):214-223. doi:10.1001/jama.2022.23924 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
