

Bilateral infraoptic origin of the anterior cerebral artery: illustrative case
- PMID: 37956417
- PMCID: PMC10651390
- DOI: 10.3171/CASE23418
Bilateral infraoptic origin of the anterior cerebral artery: illustrative case
Abstract
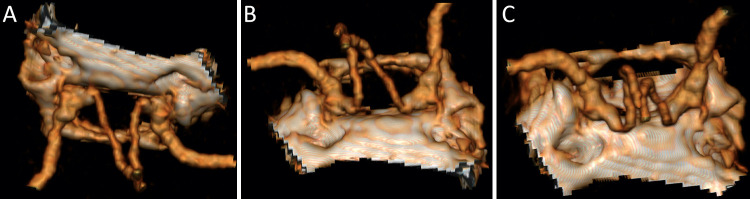
Background: A bilateral infraoptic origin of the anterior cerebral arteries (ACAs) is a rare anatomical variant that can be encountered during anterior skull base surgery. The ACAs arise from the internal carotid artery (ICA) at the level of the ophthalmic artery and course medially, traveling inferior to the ipsilateral optic nerves. Herein, the authors discuss the different configurations of the anatomical variant, its prevalence, and hypotheses leading to the variable configuration of this anomaly.
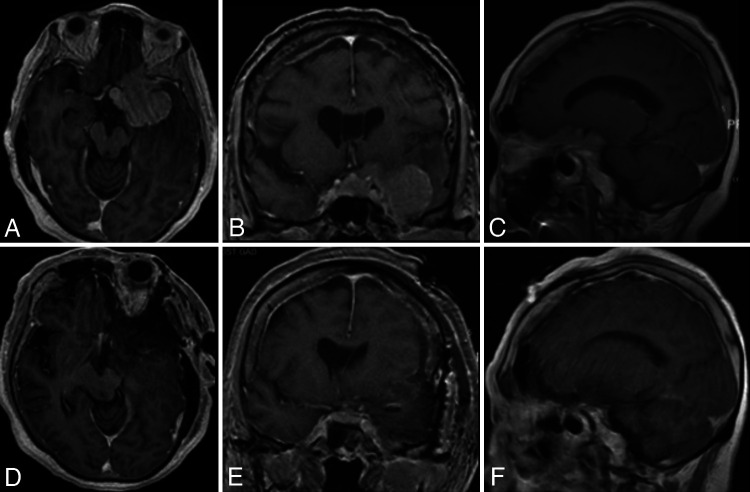
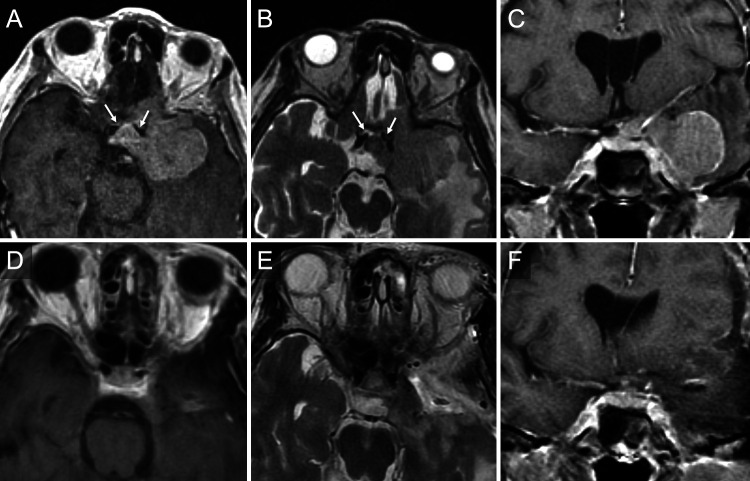
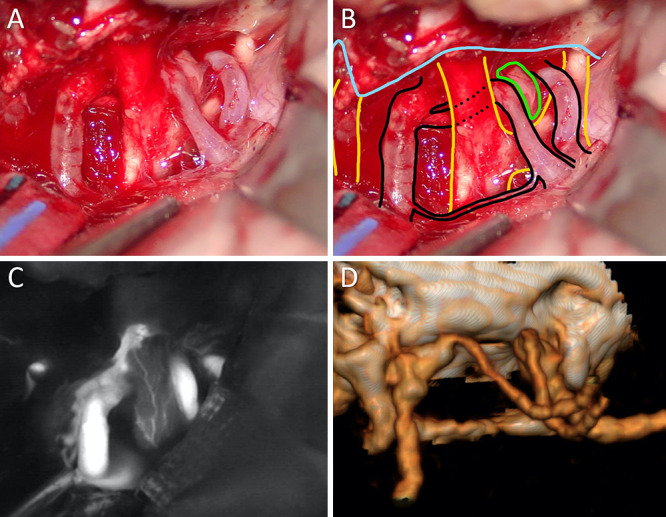
Observations: A 67-year-old woman presented with worsening dizziness over a week-long period and was found to have a large left sphenocavernous meningioma with optic, cavernous, and suprasellar extension. The tumor incorporated the left supraclinoid ICA and its branches. She underwent a left modified orbitozygomatic craniotomy for tumor resection. Early identification of the aberrant ACA anatomy was crucial in avoiding vascular injury.
Lessons: While this variant is typically encountered during the treatment of vascular pathologies-namely, intracranial aneurysms-its existence should be kept in mind during the treatment of any anterior skull base pathology. Failure to account for the presence of this variant may lead to potential intraoperative complications.
Keywords: anterior cerebral artery; cerebrovascular; meningioma; skull base surgery; skull base tumor.
Conflict of interest statement
Figures
References
-
- Osborn AG, Jacobs JM, Osborn AG. Diagnostic Cerebral Angiography. 2nd ed. Lippincott-Raven; 1999.
-
- Uchino A. Infraoptic anterior cerebral artery (ACA) versus carotid-ACA anastomosis. Surg Radiol Anat. 2017;39(8):937. - PubMed
-
- Kochar PS, Soin P, Elfatairy K. Infraoptic anterior cerebral artery or carotid-anterior cerebral artery anastomosis: a very rare embryological variation. Case series and review of literature. Clin Imaging. 2021;79:8–11. - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
