

SARS-CoV-2 Virologic Rebound With Nirmatrelvir-Ritonavir Therapy : An Observational Study
- PMID: 37956428
- PMCID: PMC10644265
- DOI: 10.7326/M23-1756
SARS-CoV-2 Virologic Rebound With Nirmatrelvir-Ritonavir Therapy : An Observational Study
Erratum in
-
Correction: SARS-CoV-2 Virologic Rebound With Nirmatrelvir-Ritonavir Therapy.Ann Intern Med. 2024 Apr;177(4):547. doi: 10.7326/L24-0045. Epub 2024 Feb 20. Ann Intern Med. 2024. PMID: 38373305 No abstract available.
Abstract
Background: Data are conflicting regarding an association between treatment of acute COVID-19 with nirmatrelvir-ritonavir (N-R) and virologic rebound (VR).
Objective: To compare the frequency of VR in patients with and without N-R treatment for acute COVID-19.
Design: Observational cohort study.
Setting: Multicenter health care system in Boston, Massachusetts.
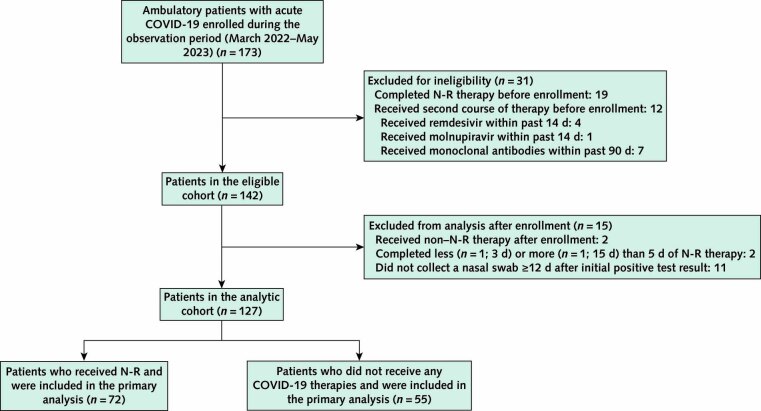
Participants: Ambulatory adults with acute COVID-19 with and without use of N-R.
Intervention: Receipt of 5 days of N-R treatment versus no COVID-19 therapy.
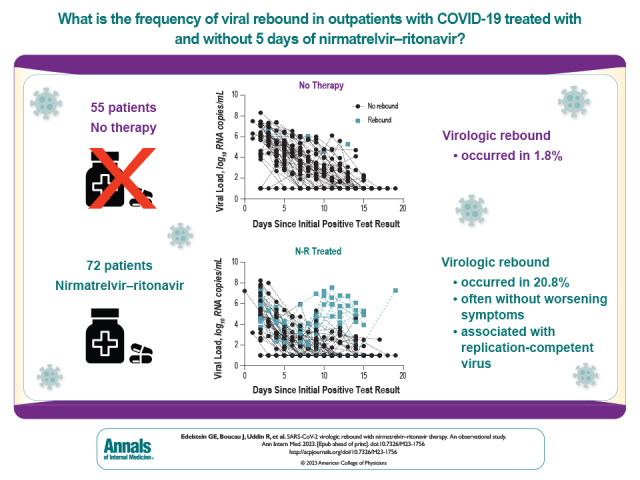
Measurements: The primary outcome was VR, defined as either a positive SARS-CoV-2 viral culture result after a prior negative result or 2 consecutive viral loads above 4.0 log10 copies/mL that were also at least 1.0 log10 copies/mL higher than a prior viral load below 4.0 log10 copies/mL.
Results: Compared with untreated persons (n = 55), those taking N-R (n = 72) were older, received more COVID-19 vaccinations, and more commonly had immunosuppression. Fifteen participants (20.8%) taking N-R had VR versus 1 (1.8%) who was untreated (absolute difference, 19.0 percentage points [95% CI, 9.0 to 29.0 percentage points]; P = 0.001). All persons with VR had a positive viral culture result after a prior negative result. In multivariable models, only N-R use was associated with VR (adjusted odds ratio, 10.02 [CI, 1.13 to 88.74]; P = 0.038). Virologic rebound was more common among those who started therapy within 2 days of symptom onset (26.3%) than among those who started 2 or more days after symptom onset (0%) (P = 0.030). Among participants receiving N-R, those who had VR had prolonged shedding of replication-competent virus compared with those who did not have VR (median, 14 vs. 3 days). Eight of 16 participants (50% [CI, 25% to 75%]) with VR also reported symptom rebound; 2 were completely asymptomatic. No post-VR resistance mutations were detected.
Limitations: Observational study design with differences between the treated and untreated groups; positive viral culture result was used as a surrogate marker for risk for ongoing viral transmission.
Conclusion: Virologic rebound occurred in approximately 1 in 5 people taking N-R, often without symptom rebound, and was associated with shedding of replication-competent virus.
Primary funding source: National Institutes of Health.
Conflict of interest statement
Figures



Update of
-
SARS-CoV-2 virologic rebound with nirmatrelvir-ritonavir therapy.medRxiv [Preprint]. 2023 Jun 27:2023.06.23.23288598. doi: 10.1101/2023.06.23.23288598. medRxiv. 2023. Update in: Ann Intern Med. 2023 Dec;176(12):1577-1585. doi: 10.7326/M23-1756. PMID: 37425934 Free PMC article. Updated. Preprint.
Comment in
-
Rebound of COVID-19 With Nirmatrelvir-Ritonavir Antiviral Therapy.Ann Intern Med. 2023 Dec;176(12):1672-1673. doi: 10.7326/M23-2887. Epub 2023 Nov 14. Ann Intern Med. 2023. PMID: 37956432 Free PMC article.
References
-
- National Institutes of Health. COVID-19 Treatment Guidelines: Therapeutic Management of Nonhospitalized Adults With COVID-19. Updated 21 July 2023. Accessed at www.covid19treatmentguidelines.nih.gov/management/clinical-management-of... on 18 October 2023.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous