

Incidence and Determinants of Acute Kidney Injury after Prone Positioning in Severe COVID-19 Acute Respiratory Distress Syndrome
- PMID: 37958047
- PMCID: PMC10647784
- DOI: 10.3390/healthcare11212903
Incidence and Determinants of Acute Kidney Injury after Prone Positioning in Severe COVID-19 Acute Respiratory Distress Syndrome
Abstract
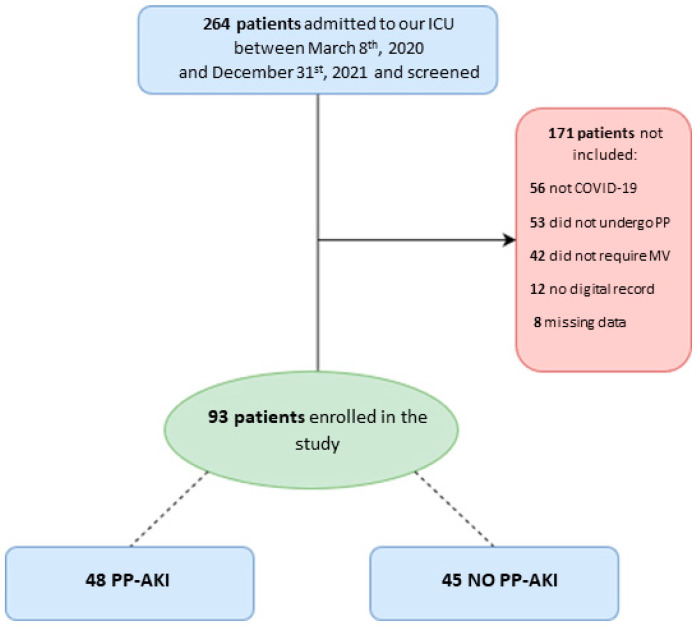
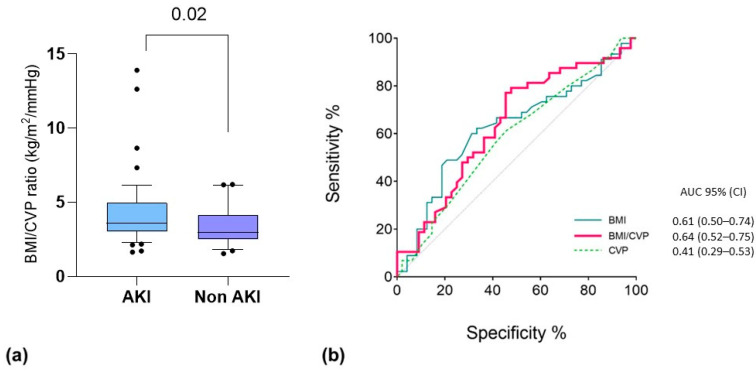
(1) Background: Acute kidney injury (AKI) is common among critically ill COVID-19 patients, but its temporal association with prone positioning (PP) is still unknown, and no data exist on the possibility of predicting PP-associated AKI from bedside clinical variables. (2) Methods: We analyzed data from 93 COVID-19-related ARDS patients who underwent invasive mechanical ventilation (IMV) and at least one PP cycle. We collected hemodynamic variables, respiratory mechanics, and circulating biomarkers before, during, and after the first PP cycle. PP-associated AKI (PP-AKI) was defined as AKI diagnosed any time from the start of PP to 48 h after returning to the supine position. A t-test for independent samples was used to test for the differences between groups, while binomial logistical regression was performed to assess variables independently associated with PP-associated AKI. (3) Results: A total of 48/93 (52%) patients developed PP-AKI, with a median onset at 24 [13.5-44.5] hours after starting PP. No significant differences in demographic characteristics between groups were found. Before starting the first PP cycle, patients who developed PP-AKI had a significantly lower cumulative fluid balance (CFB), even when normalized for body weight (p = 0.006). Central venous pressure (CVP) values, measured before the first PP (OR 0.803, 95% CI [0.684-0.942], p = 0.007), as well as BMI (OR 1.153, 95% CI = [1.013-1.313], p = 0.031), were independently associated with the development of PP-AKI. In the multivariable regression analysis, a lower CVP before the first PP cycle was independently associated with ventilator-free days (OR 0.271, 95% CI [0.123-0.936], p = 0.011) and with ICU mortality (OR:0.831, 95% CI [0.699-0.989], p = 0.037). (4) Conclusions: Acute kidney injury occurs frequently in invasively ventilated severe COVID-19 ARDS patients undergoing their first prone positioning cycle. Higher BMI and lower CVP before PP are independently associated with the occurrence of AKI during prone positioning.
Keywords: acute kidney injury; acute respiratory distress syndrome; central venous pressure; mechanical ventilation; prone positioning.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Zanella A., Florio G., Antonelli M., Bellani G., Berselli A., Bove T., Cabrini L., Carlesso E., Castelli G.P., Cecconi M., et al. Time course of risk factors associated with mortality of 1260 critically ill patients with COVID-19 admitted to 24 Italian intensive care units. Intensive Care Med. 2021;47:995–1008. doi: 10.1007/s00134-021-06495-y. - DOI - PMC - PubMed
-
- Lumlertgul N., Pirondini L., Cooney E., Kok W., Gregson J., Camporota L., Lane K., Leach R., Ostermann M. Acute kidney injury prevalence, progression and long-term outcomes in critically ill patients with COVID-19: A cohort study. Ann. Intensiv. Care. 2021;11:123. doi: 10.1186/s13613-021-00914-5. - DOI - PMC - PubMed
-
- Alhazzani W., Møller M.H., Arabi Y.M., Loeb M., Gong M.N., Fan E., Oczkowski S., Levy M.M., Derde L., Dzierba A., et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19) Intensive Care Med. 2020;46:854–887. doi: 10.1007/s00134-020-06022-5. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
