

Effectiveness of Palliative Care before Death in Reducing Emergency Care Utilization for Patients with Terminal Cancer and Trends in the Utilization of Palliative Care from 2005-2018
- PMID: 37958051
- PMCID: PMC10647500
- DOI: 10.3390/healthcare11212907
Effectiveness of Palliative Care before Death in Reducing Emergency Care Utilization for Patients with Terminal Cancer and Trends in the Utilization of Palliative Care from 2005-2018
Abstract
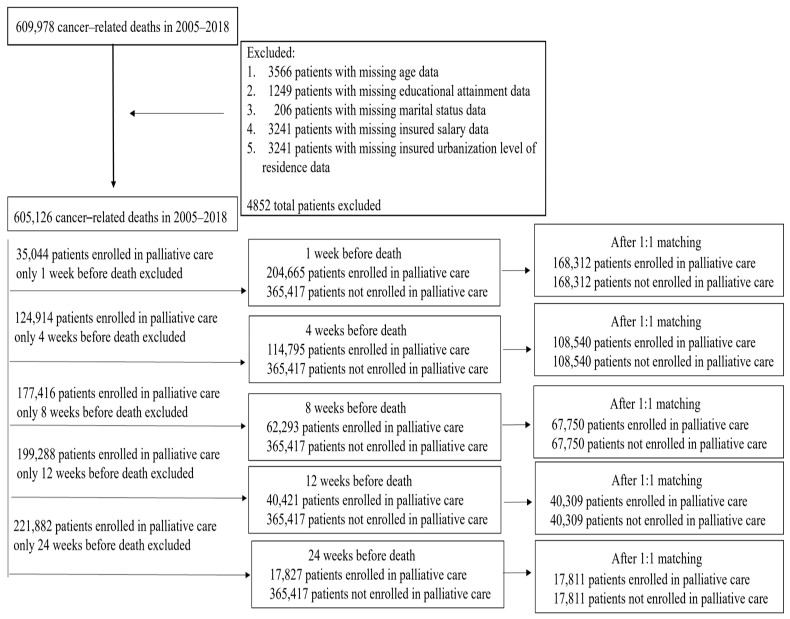
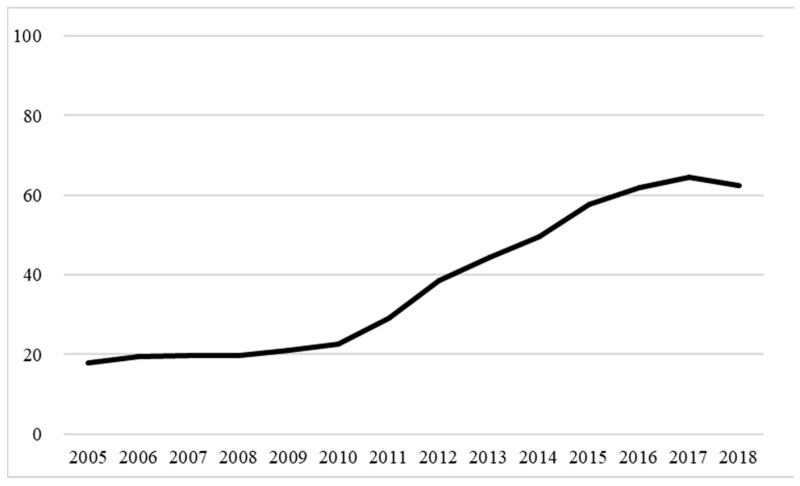
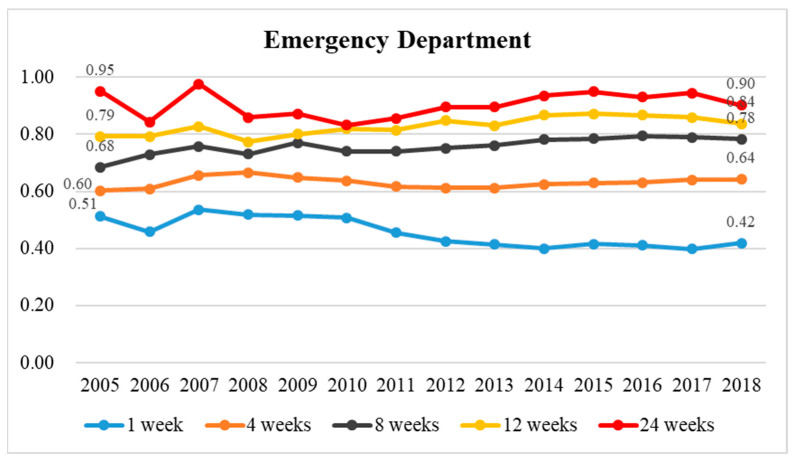
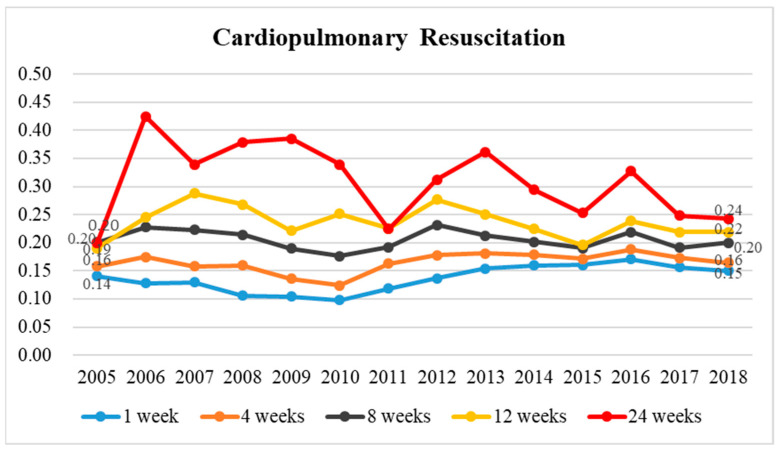
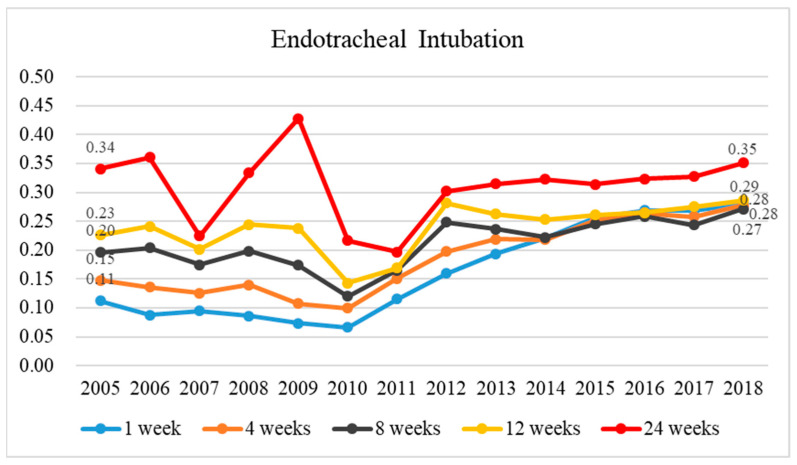
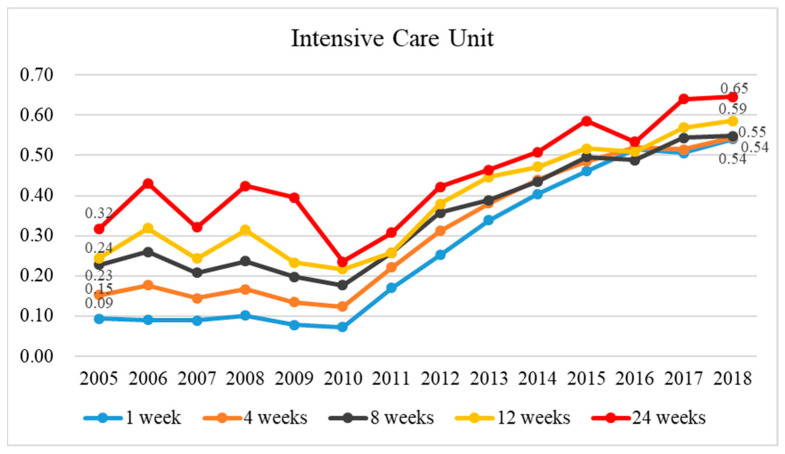
This retrospective cohort study aimed to examine the effect of palliative care for patients with terminal cancer on healthcare utilization. The National Health Insurance (NHI) Research Database and death certificates were utilized to identify patients who died of cancer between 2005 and 2018. The number of terminal cancer patients between 2005 and 2018 was 605,126. Propensity score matching and conditional logistic regression were performed. The odds ratios (ORs) for "emergency care utilization", "CPR", "endotracheal intubation", and "ICU admission" were significantly lower for enrolled patients regardless of enrollment time compared to unenrolled patients. Compared to unenrolled patients, the OR for "emergency care utilization" increased from 0.34 to 0.68, the OR for "CPR use" increased from 0.13 to 0.26, the OR for "intubation" increased from 0.15 to 0.26, and the OR for "ICU admission" increased from 0.27 to 0.40 in enrolled patients. Between 2005 and 2010, CPR utilization, intubation, and ICU admission in patients enrolled in palliative care declined each year. Since the inclusion of palliative care in NHI (from 2010 onward), its utilization has increased slightly each year. Patients with terminal cancer enrolled in palliative care consume fewer medical resources before death than unenrolled patients; however, the difference decreases with longer times before death.
Keywords: CPR (cardiopulmonary resuscitation); ICU (intensive care unit) admission; emergency care utilization; endotracheal intubation; palliative care; terminal cancer patients.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Trends of Utilization of Palliative Care and Aggressive End-of-Life Care for Patients Who Died of Cancers and Those Who Died of Noncancer Diseases in Hospitals.J Pain Symptom Manage. 2020 Dec;60(6):1136-1143. doi: 10.1016/j.jpainsymman.2020.06.037. Epub 2020 Jun 30. J Pain Symptom Manage. 2020. PMID: 32619671
-
Early Palliative Care Reduces End-of-Life Intensive Care Unit (ICU) Use but Not ICU Course in Patients with Advanced Cancer.Oncologist. 2017 Mar;22(3):318-323. doi: 10.1634/theoncologist.2016-0227. Epub 2017 Feb 20. Oncologist. 2017. PMID: 28220023 Free PMC article.
-
Palliative Family Conference Reduces the Risk of Death in Intensive Care Units and Cardiopulmonary Resuscitation at End of Life.J Palliat Med. 2022 Jul;25(7):1050-1056. doi: 10.1089/jpm.2021.0546. Epub 2022 Mar 28. J Palliat Med. 2022. PMID: 35349365
-
Effects of the Time of Hospice and Palliative Care Enrollment before Death on Morphine, Length of Stay, and Healthcare Expense in Patients with Cancer in Taiwan.Healthcare (Basel). 2023 Oct 31;11(21):2867. doi: 10.3390/healthcare11212867. Healthcare (Basel). 2023. PMID: 37958010 Free PMC article.
-
Intensive care utilization in patients with end-stage liver disease: A population-based comparative study of cohorts with and without comorbid hepatocellular carcinoma in taiwan.EClinicalMedicine. 2020 May 20;22:100357. doi: 10.1016/j.eclinm.2020.100357. eCollection 2020 May. EClinicalMedicine. 2020. PMID: 32462117 Free PMC article.
Cited by
-
Influence of Hospice Palliative Care on Medical Service Usage in Prolonged Mechanical Ventilation Cases: A Nationwide Cohort Study.Respir Care. 2024 Nov 18;69(12):1523-1533. doi: 10.4187/respcare.11587. Respir Care. 2024. PMID: 39256001
-
Effects of early palliative care intervention on medical resource use among end-of-life patients.Int J Qual Health Care. 2025 Jan 9;37(1):mzae119. doi: 10.1093/intqhc/mzae119. Int J Qual Health Care. 2025. PMID: 39739420 Free PMC article.
References
-
- World Health Organization Cancer. 2022. [(accessed on 3 February 2022)]. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer.
Grants and funding
LinkOut - more resources
Full Text Sources
