

Transjugular Intrahepatic Portosystemic Shunt: Devices Evolution, Technical Tips and Future Perspectives
- PMID: 37959225
- PMCID: PMC10650044
- DOI: 10.3390/jcm12216758
Transjugular Intrahepatic Portosystemic Shunt: Devices Evolution, Technical Tips and Future Perspectives
Abstract
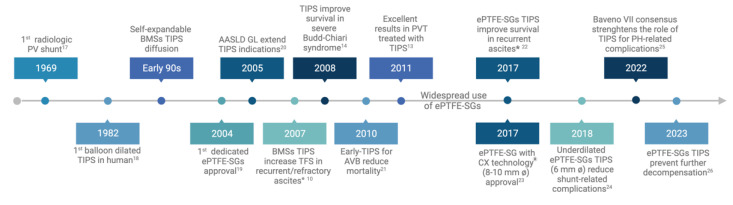
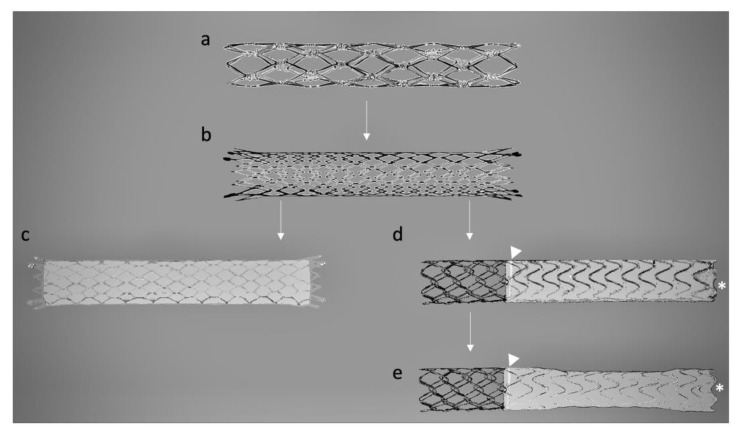
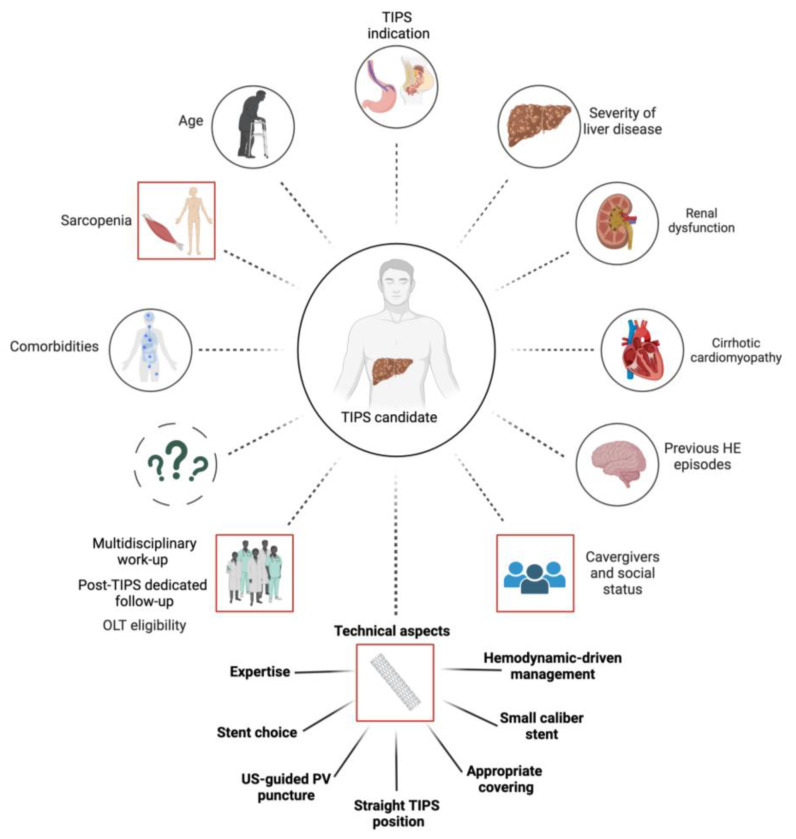
Portal hypertension (PH) constitutes a pivotal factor in the progression of cirrhosis, giving rise to severe complications and a diminished survival rate. The transjugular intrahepatic portosystemic shunt (TIPS) procedure has undergone significant evolution, with advancements in stent technology assuming a central role in managing PH-related complications. This review aims to outline the progression of TIPS and emphasizes the significant influence of stent advancement on its effectiveness. Initially, the use of bare metal stents (BMSs) was limited due to frequent dysfunction. However, the advent of expanding polytetrafluoroethylene-covered stent grafts (ePTFE-SGs) heralded a transformative era, greatly enhancing patency rates. Further innovation culminated in the creation of ePTFE-SGs with controlled expansion, enabling precise adjustment of TIPS diameters. Comparative analyses demonstrated the superiority of ePTFE-SGs over BMSs, resulting in improved patency, fewer complications, and higher survival rates. Additional technical findings highlight the importance of central stent placement and adequate stent length, as well as the use of smaller calibers to reduce the risk of shunt-related complications. However, improving TIPS through technical means alone is inadequate for optimizing patient outcomes. An extensive understanding of hemodynamic, cardiac, and systemic factors is required to predict outcomes and tailor a personalized approach. Looking forward, the ongoing progress in SG technology, paired with the control of clinical factors that can impact outcomes, holds the promise of reshaping the management of PH-related complications in cirrhosis.
Keywords: complications; patency; personalized medicine; portal hypertension; stent technology; transjugular intrahepatic portosystemic shunt (TIPS).
Conflict of interest statement
A.C. is a consultant for Jazz Pharmaceuticals; F.S. is a consultant for Echosens, a lecturer for Echosens and W.L. Gore and Cook Medical, and a recipient of an non-profit grants from W.L. Gore and Cook Medical.
Figures
References
-
- Ripoll C., Groszmann R., Garcia-Tsao G., Grace N., Burroughs A., Planas R., Escorsell A., Garcia-Pagan J.C., Makuch R., Patch D., et al. Hepatic Venous Pressure Gradient Predicts Clinical Decompensation in Patients with Compensated Cirrhosis. Gastroenterology. 2007;133:481–488. doi: 10.1053/j.gastro.2007.05.024. - DOI - PubMed
-
- Vizzutti F., Schepis F., Arena U., Fanelli F., Gitto S., Aspite S., Turco L., Dragoni G., Laffi G., Marra F. Transjugular Intrahepatic Portosystemic Shunt (TIPS): Current Indications and Strategies to Improve the Outcomes. Intern. Emerg. Med. 2020;15:37–48. doi: 10.1007/s11739-019-02252-8. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
