

Patient Position in Operative Endoscopy
- PMID: 37959286
- PMCID: PMC10649681
- DOI: 10.3390/jcm12216822
Patient Position in Operative Endoscopy
Abstract
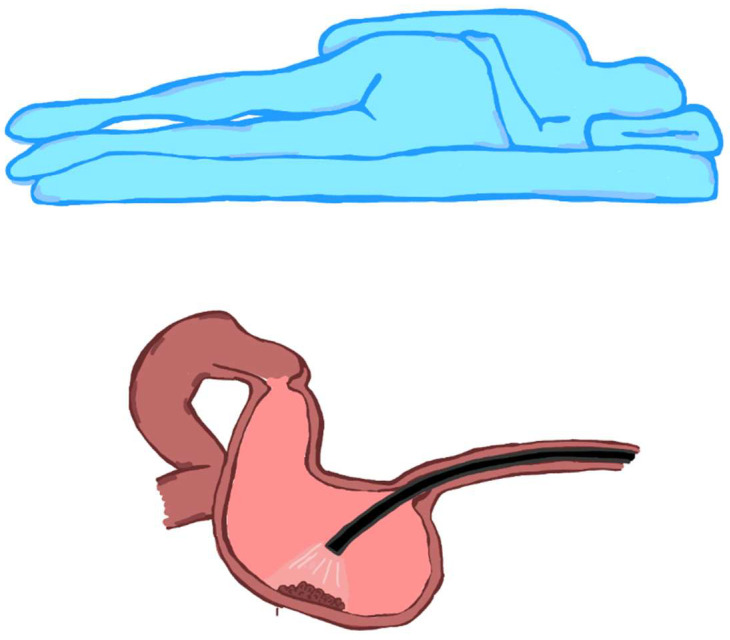
It is well known by surgeons that patient positioning is fundamental to exposing the organs when performing an operation via laparoscopy, as gravity can help move the organs and facilitate the exposure of the surgical site. But is it also important for endoscopic procedures? This paper examines various types of endoscopic operations and addresses the issue of the patient's position. The patient's position can be changed not only by rotating the patient along the head-toe axis but also by tilting the surgical bed, as is undertaken during laparoscopic surgical procedures. In particular, it is useful to take into account the effect of gravity on lesion exposure, tumour traction during dissection, crushing by body weight, risk of sample drop, risk of damage to adjacent organs, and anatomical exposure for procedures with radiological support. The endoscopist should always keep in mind the patient's anatomy and the position of the endoscope during operative procedures, not limited to considering only intraluminal vision.
Keywords: ERCP; ESD; POEM; colonoscopy; operative endoscopy; patient position; prone; supine.
Conflict of interest statement
The authors declare no conflict of interest.
Figures






References
-
- Feix B.S. Anaesthesia in the prone position. Contin. Educ. Anaesth. Crit. Care Pain. 2014;14:291–297. doi: 10.1093/bjaceaccp/mku001. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
