

The Role of Chest Compressions on Ventilation during Advanced Cardiopulmonary Resuscitation
- PMID: 37959385
- PMCID: PMC10647836
- DOI: 10.3390/jcm12216918
The Role of Chest Compressions on Ventilation during Advanced Cardiopulmonary Resuscitation
Abstract
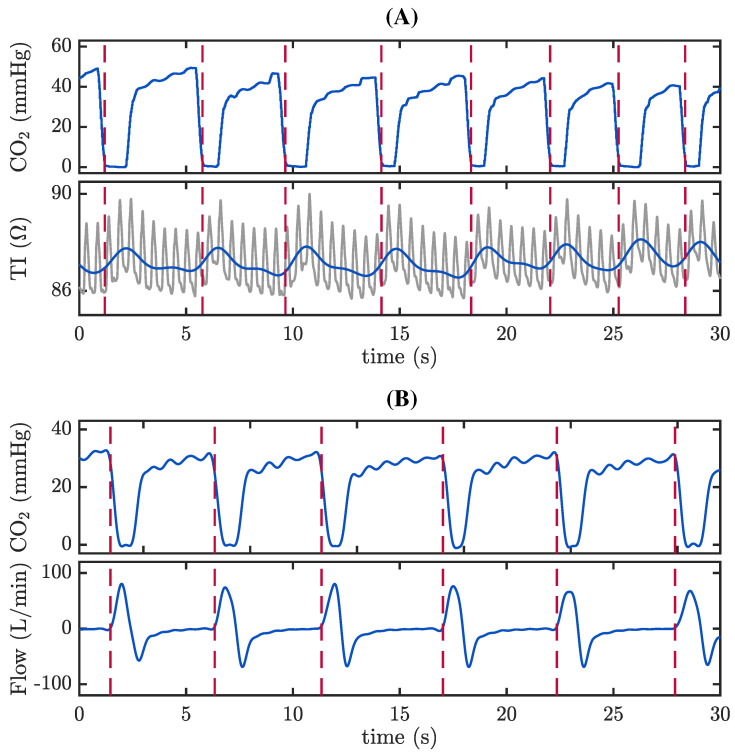
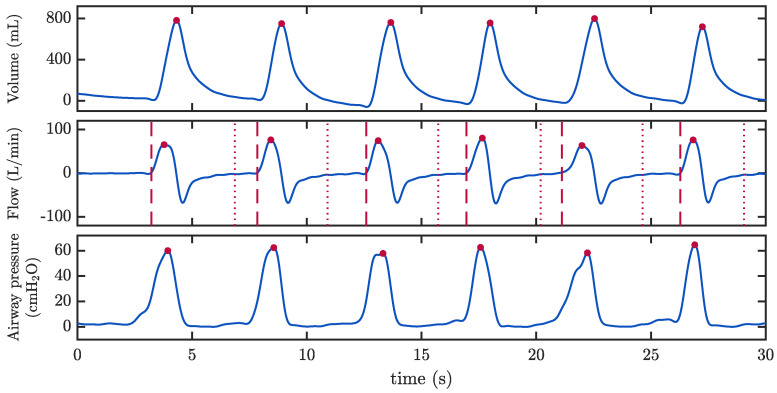
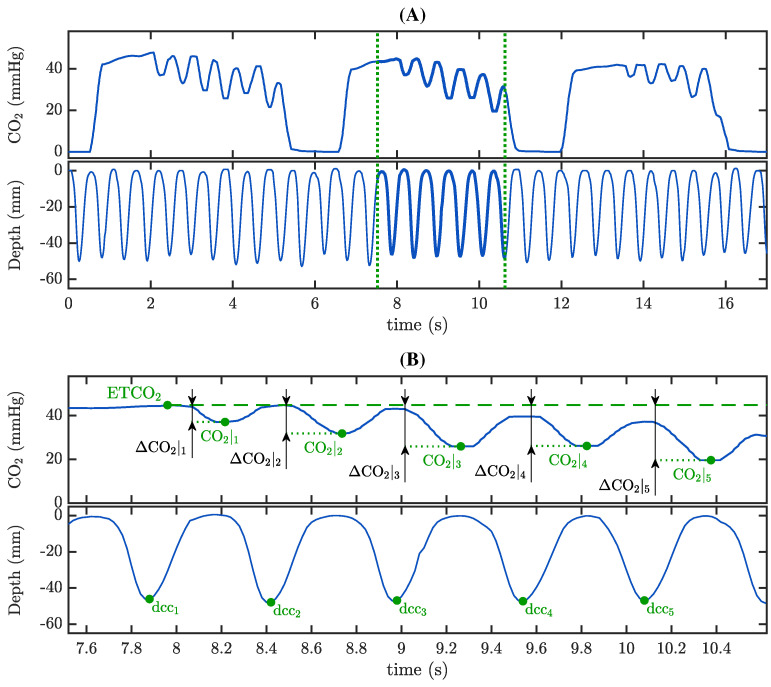
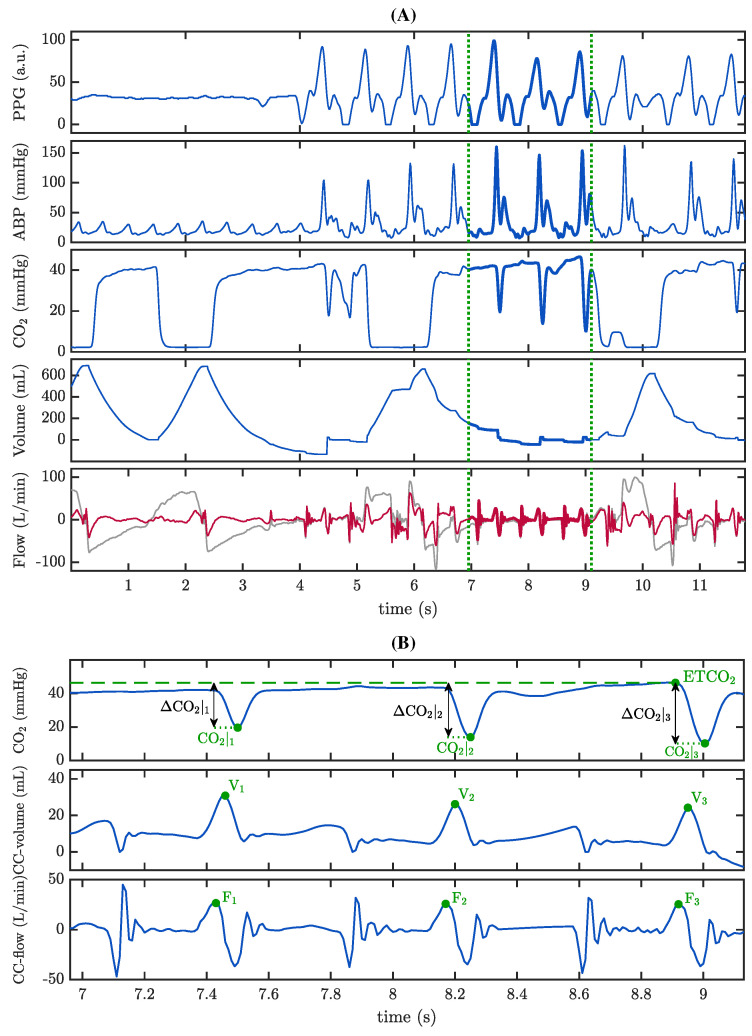
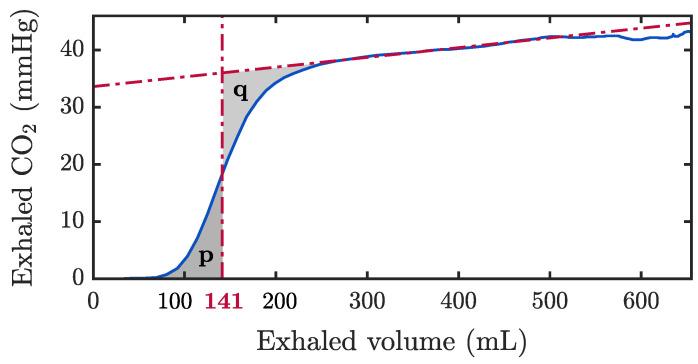
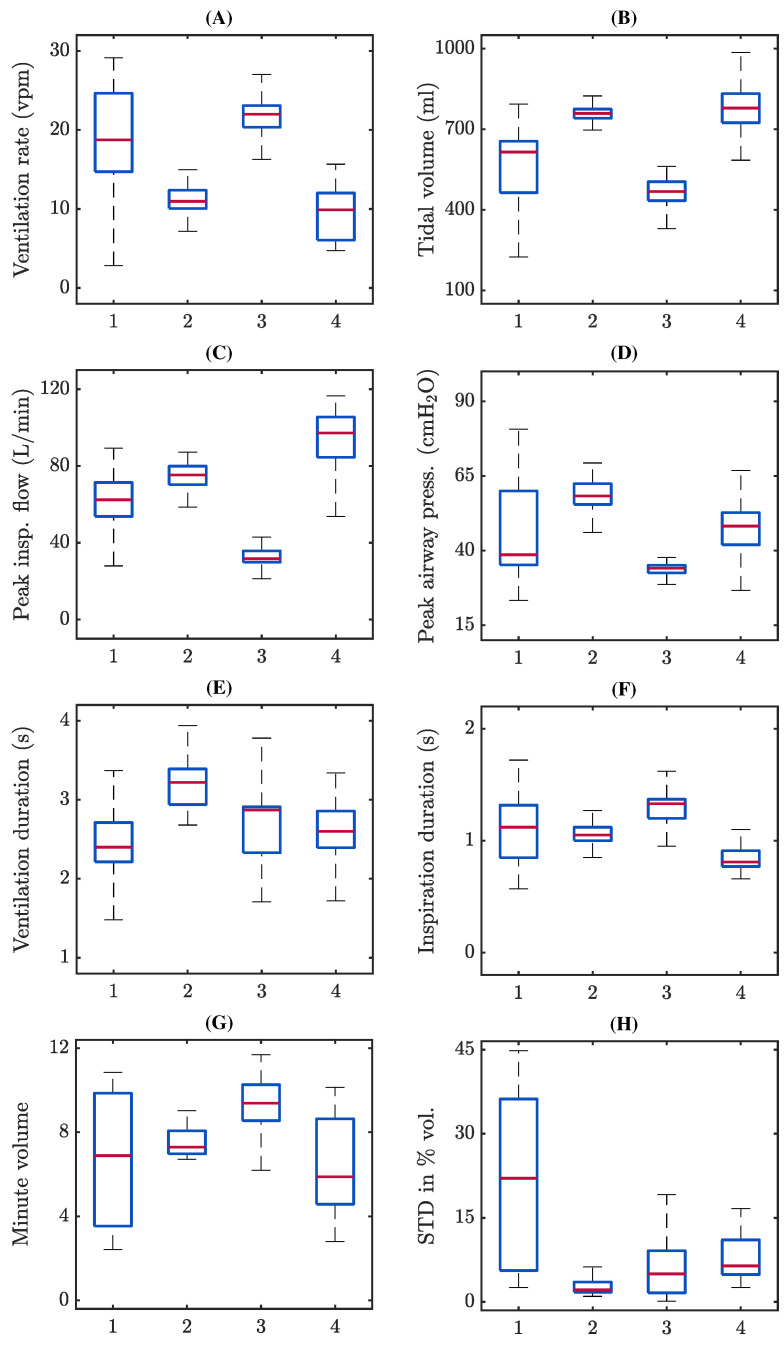
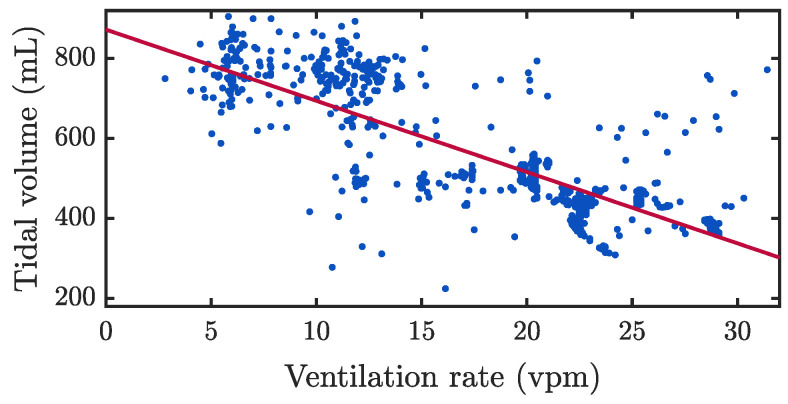
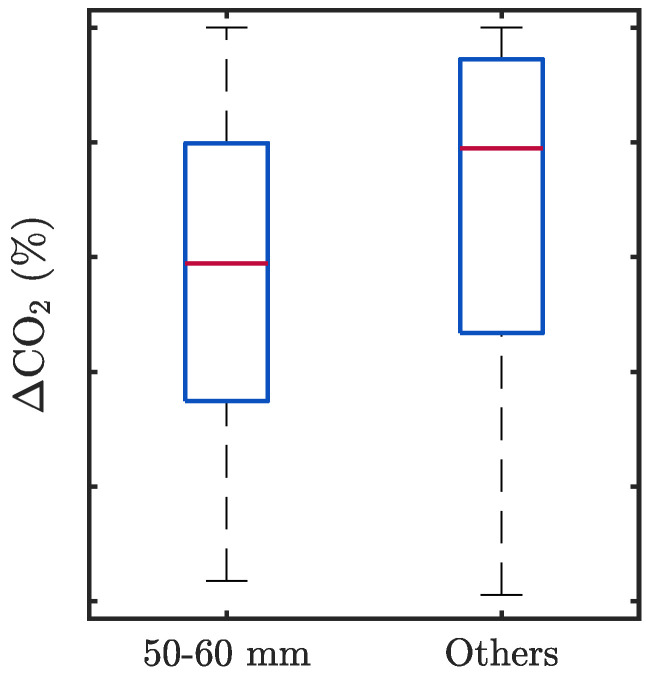
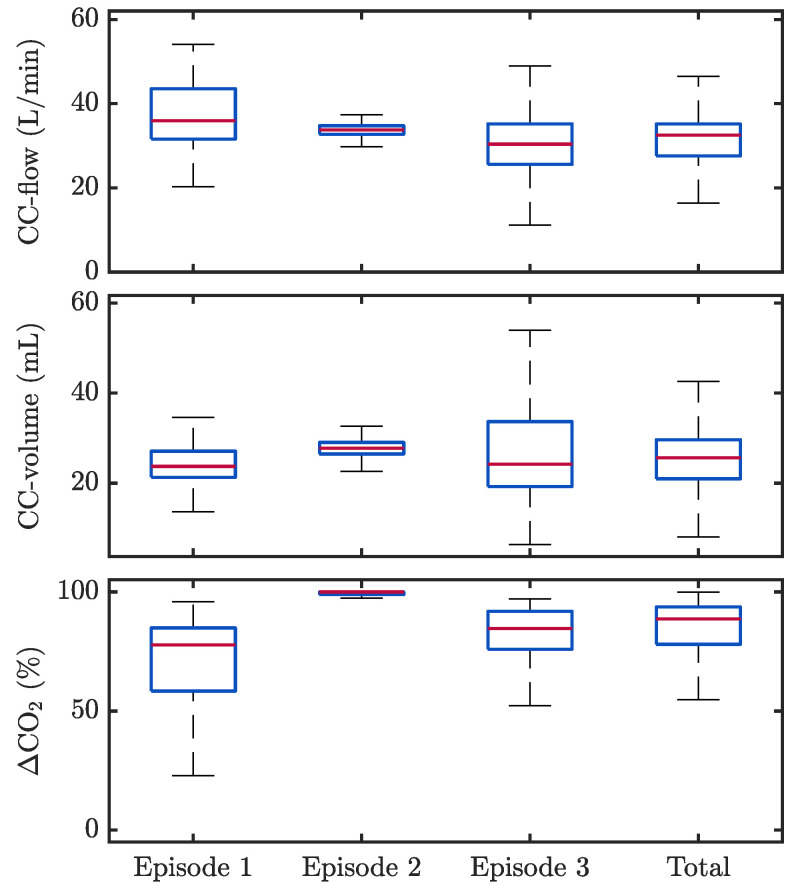
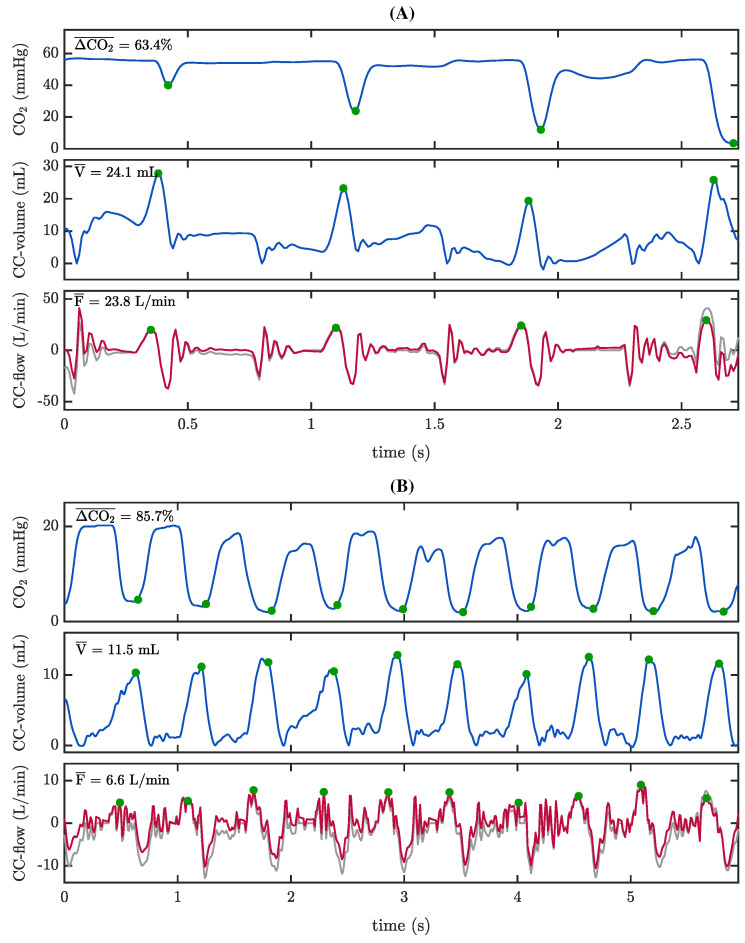
Background: There is growing interest in the quality of manual ventilation during cardiopulmonary resuscitation (CPR), but accurate assessment of ventilation parameters remains a challenge. Waveform capnography is currently the reference for monitoring ventilation rate in intubated patients, but fails to provide information on tidal volumes and inspiration-expiration timing. Moreover, the capnogram is often distorted when chest compressions (CCs) are performed during ventilation compromising its reliability during CPR. Our main purpose was to characterize manual ventilation during CPR and to assess how CCs may impact on ventilation quality. Methods: Retrospective analysis were performed of CPR recordings fromtwo databases of adult patients in cardiac arrest including capnogram, compression depth, and airway flow, pressure and volume signals. Using automated signal processing techniques followed by manual revision, individual ventilations were identified and ventilation parameters were measured. Oscillations on the capnogram plateau during CCs were characterized, and its correlation with compression depth and airway volume was assessed. Finally, we identified events of reversed airflow caused by CCs and their effect on volume and capnogram waveform. Results: Ventilation rates were higher than the recommended 10 breaths/min in 66.7% of the cases. Variability in ventilation rates correlated with the variability in tidal volumes and other ventilatory parameters. Oscillations caused by CCs on capnograms were of high amplitude (median above 74%) and were associated with low pseudo-volumes (median 26 mL). Correlation between the amplitude of those oscillations with either the CCs depth or the generated passive volumes was low, with correlation coefficients of -0.24 and 0.40, respectively. During inspiration and expiration, reversed airflow events caused opposed movement of gases in 80% of ventilations. Conclusions: Our study confirmed lack of adherence between measured ventilation rates and the guideline recommendations, and a substantial dispersion in manual ventilation parameters during CPR. Oscillations on the capnogram plateau caused by CCs did not correlate with compression depth or associated small tidal volumes. CCs caused reversed flow during inspiration, expiration and in the interval between ventilations, sufficient to generate volume changes and causing oscillations on capnogram. Further research is warranted to assess the impact of these findings on ventilation quality during CPR.
Keywords: advanced life support (ALS); airway flow; cardiopulmonary resuscitation (CPR); chest compressions; tidal volume; ventilation; ventilation rate.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Meaney P.A., Bobrow B.J., Mancini M.E., Christenson J., De Caen A.R., Bhanji F., Abella B.S., Kleinman M.E., Edelson D.P., Berg R.A., et al. Cardiopulmonary resuscitation quality: Improving cardiac resuscitation outcomes both inside and outside the hospital: A consensus statement from the American Heart Association. Circulation. 2013;128:417–435. doi: 10.1161/CIR.0b013e31829d8654. - DOI - PubMed
-
- Idris A.H., Banner M.J., Wenzel V., Fuerst R.S., Becker L.B., Melker R.J. Ventilation caused by external chest compression is unable to sustain effective gas exchange during CPR: A comparison with mechanical ventilation. Resuscitation. 1994;28:143–150. doi: 10.1016/0300-9572(94)90087-6. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
