

Connecting the disconnected: Leveraging an in-home team member for video visits for older adults
- PMID: 37960887
- PMCID: PMC11188997
- DOI: 10.1111/jgs.18663
Connecting the disconnected: Leveraging an in-home team member for video visits for older adults
Abstract
Background: Older adults are interested and able to complete video visits, but often require coaching and practice to succeed. Data show a widening digital divide between older and younger adults using video visits. We conducted a qualitative feasibility study to investigate these gaps via ethnographic methods, including a team member in older participants' homes.
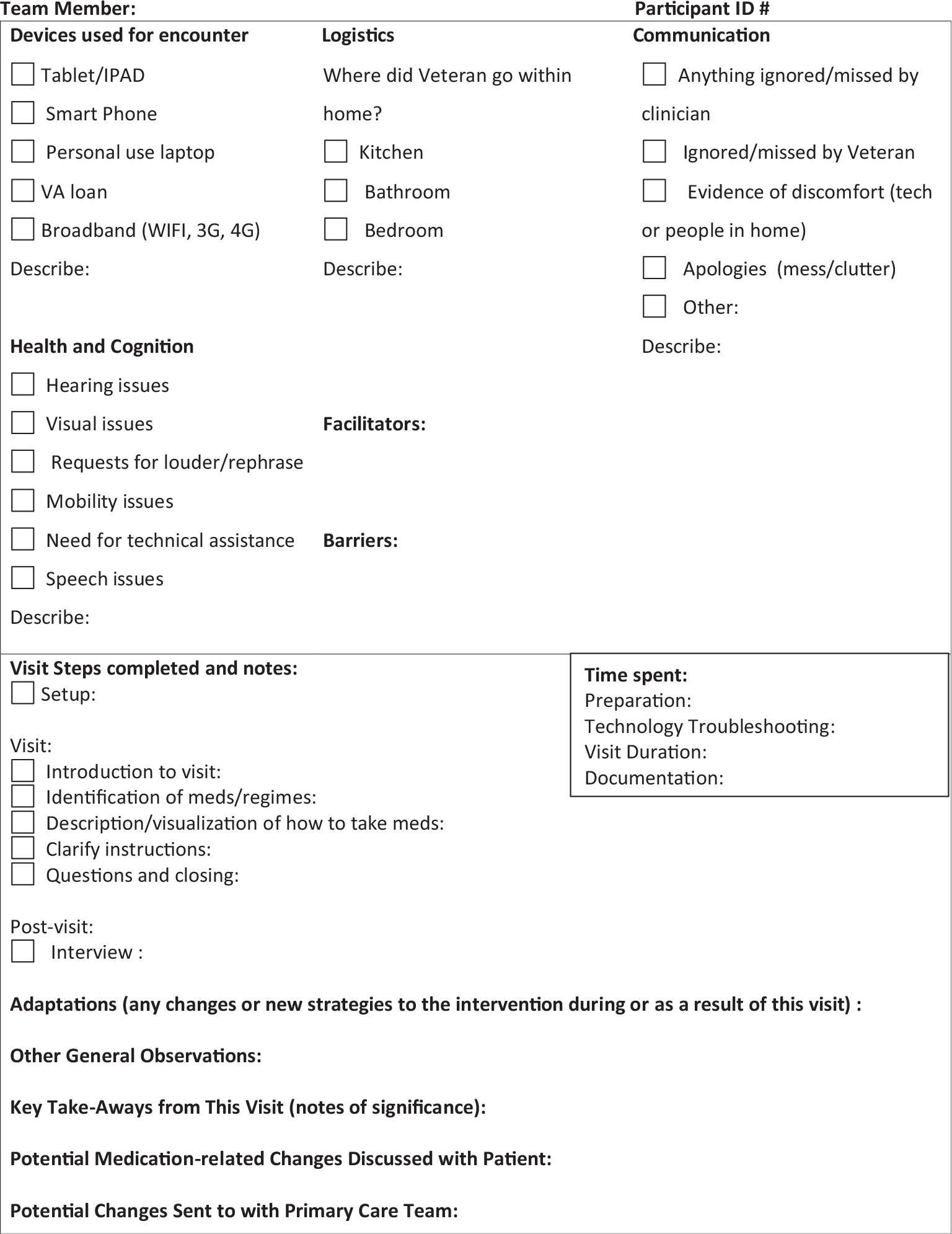
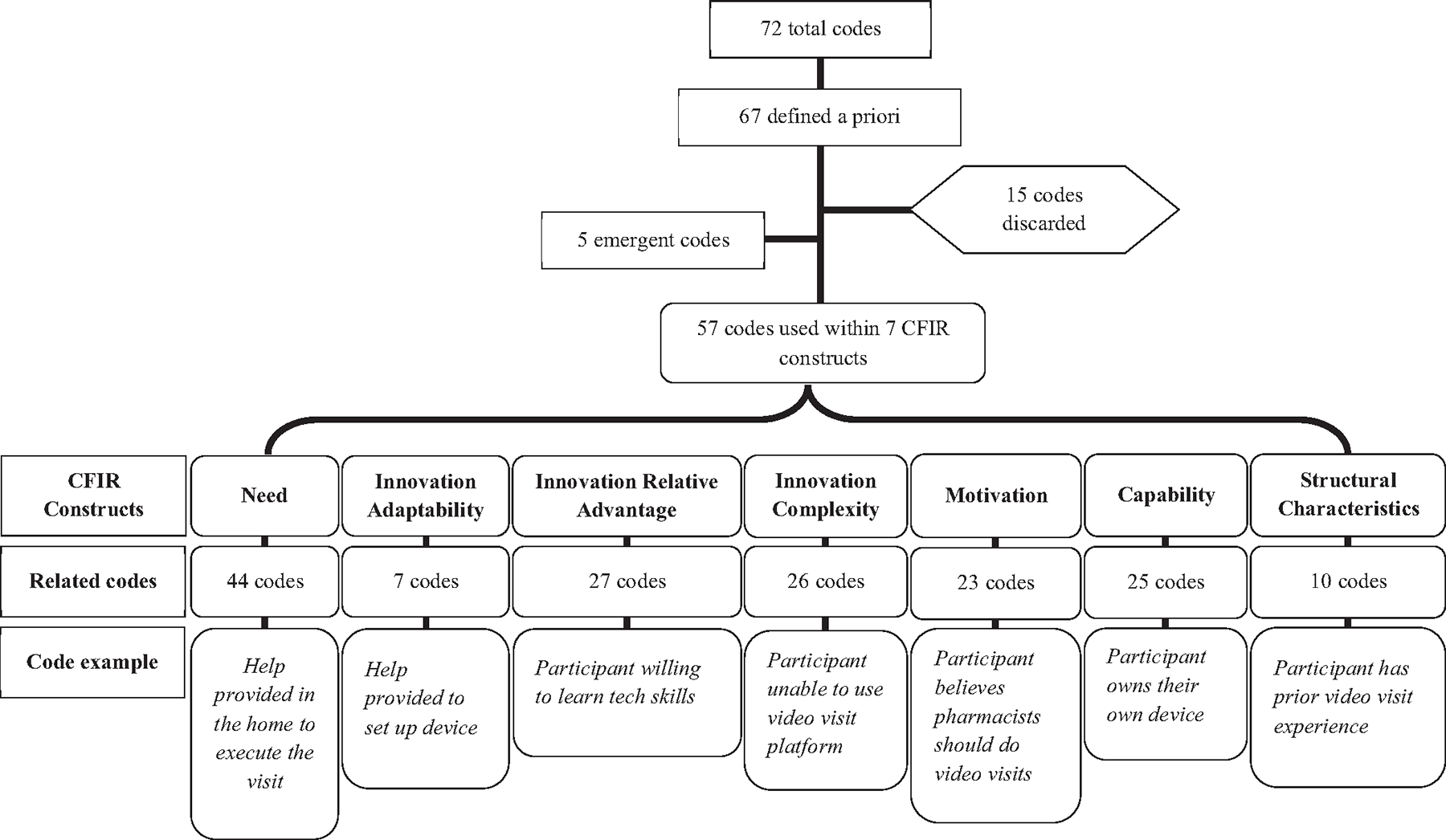
Methods: This ethnographic feasibility study included a virtual medication reconciliation visit with a clinical pharmacist for Veterans aged 65 and older taking 5 or more medications. An in-home study team member joined the participant and recorded observations in structured fieldnotes derived from the Updated Consolidated Framework for Implementation Research and Age-Friendly Health Systems. Fieldnotes included behind-the-scenes facilitators, barriers, and solutions to challenges before and during the visits. We conducted a thematic analysis of these observations and matched themes to implementation solutions from the Expert Recommendations for Implementing Change.
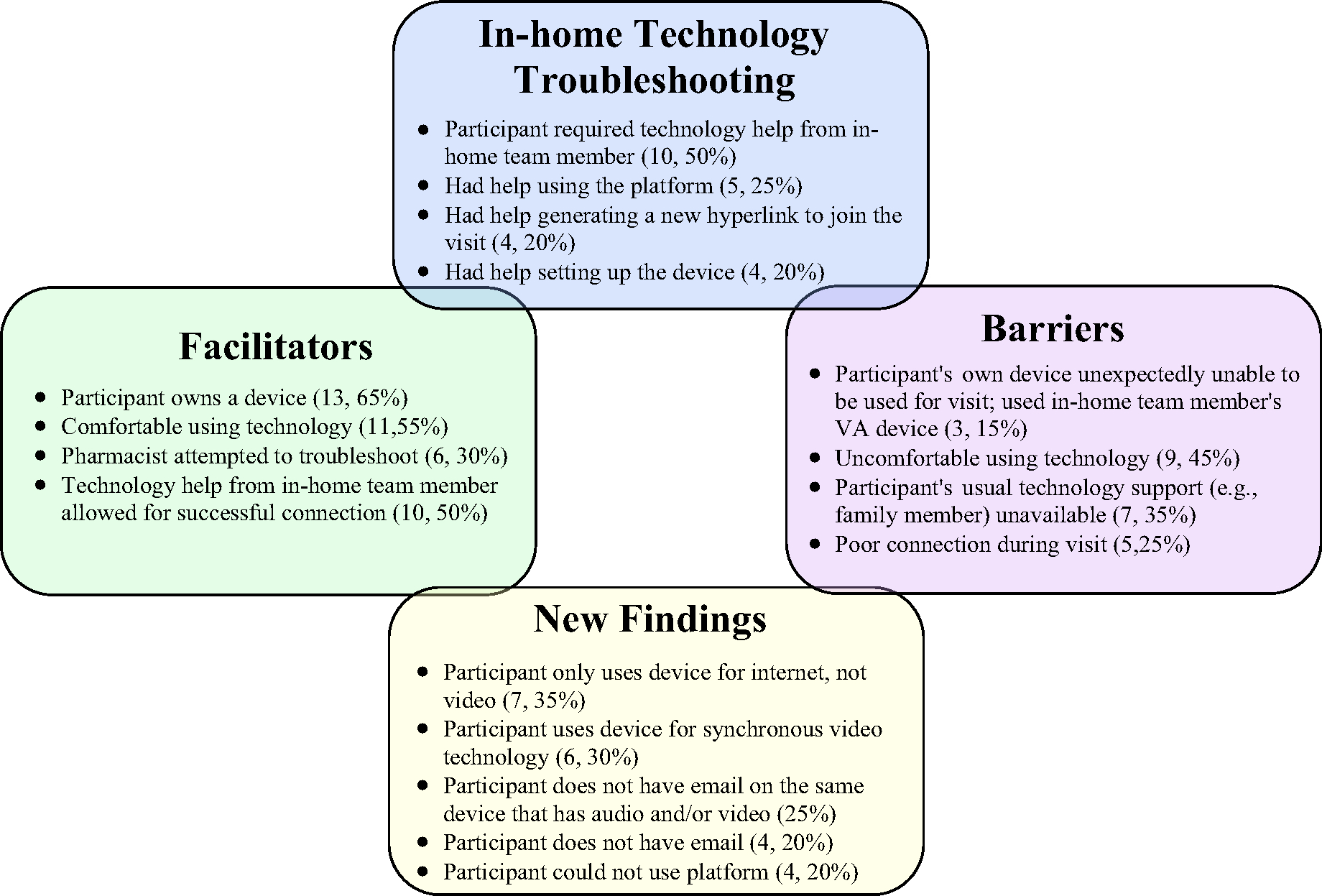
Results: Twenty participants completed a video visit. Participants were 74 years old (range 68-80) taking 12 daily medications (range 7-24). Challenges occurred in half of the visits and took the in-home team member and/or pharmacist an average of 10 minutes to troubleshoot. Challenges included notable new findings, such as that half of the participants required technology assistance for challenges that would not have been able to be solved by the pharmacist virtually. Furthermore, although many participants had a device or had used video visits before, some did not have a single device with video, audio, Internet, and access to their email username and password.
Conclusions: Clinicians may apply these evidence-based implementation solutions to their approach to video visits with older adults, including having a team member join the visit before the clinician, involving tech-savvy family members, ensuring the device works with the visit platform ahead of time, and creating a troubleshooting guide from our common challenges.
Keywords: geriatrics; home telehealth; telehealth; video visit; virtual care.
© 2023 The American Geriatrics Society. This article has been contributed to by U.S. Government employees and their work is in the public domain in the USA.
Conflict of interest statement
CONFLICT OF INTEREST STATEMENT
The authors have no conflicts to declare.
Figures
References
-
- Telehealth was critical for providing services to Medicare beneficiaries during the first year of the COVID-19 pandemic. Accessed April 25, 2023. https://oig.hhs.gov/oei/reports/OEI-02-20-00520.asp
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
