

A randomized, double-blind phase 1b study evaluating the safety, tolerability, pharmacokinetics and pharmacodynamics of the NLRP3 inhibitor selnoflast in patients with moderate to severe active ulcerative colitis
- PMID: 37962000
- PMCID: PMC10644327
- DOI: 10.1002/ctm2.1471
A randomized, double-blind phase 1b study evaluating the safety, tolerability, pharmacokinetics and pharmacodynamics of the NLRP3 inhibitor selnoflast in patients with moderate to severe active ulcerative colitis
Abstract
Background: The NLRP3 inflammasome drives release of pro-inflammatory cytokines including interleukin (IL)-1β and IL-18 and is a potential target for ulcerative colitis (UC). Selnoflast (RO7486967) is an orally active, potent, selective and reversible small molecule NLRP3 inhibitor. We conducted a randomized, placebo-controlled Phase 1b study to assess the safety, tolerability, pharmacokinetics (PK) and pharmacodynamics (PD) of selnoflast.
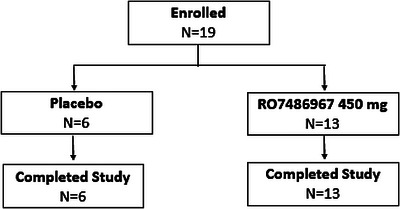
Methods: Nineteen adults with previous diagnosis of UC and current active moderate to severe disease were randomized 2:1 to selnoflast or placebo for 7 days. A dose of 450 mg QD (once daily) was selected to achieve 90% IL-1β inhibition in plasma and colon tissue. Consecutive blood, sigmoid colon biopsies and stool samples were analyzed for a variety of PD markers. Safety and PK were also evaluated.
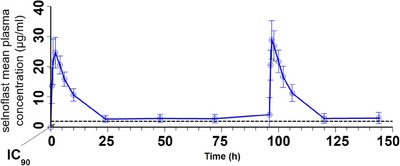
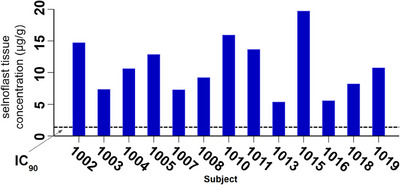
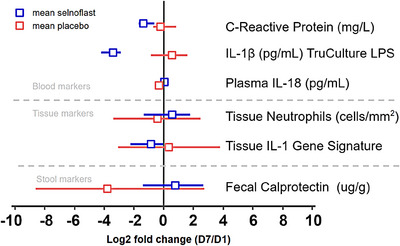
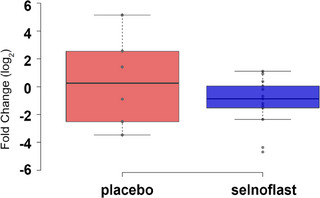
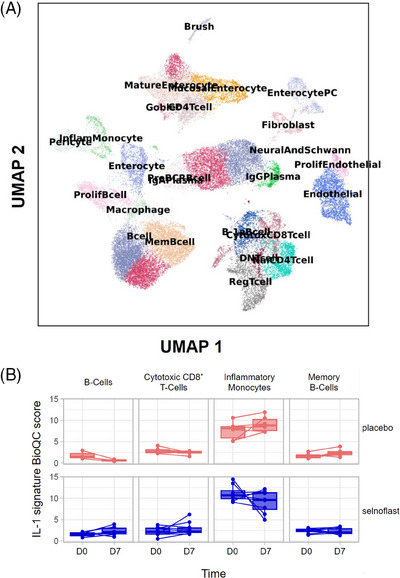
Results: Selnoflast was well-tolerated. Plasma concentrations increased rapidly after oral administration, reaching Tmax 1 h post-dose. Mean plasma concentrations stayed above the IL-1β IC90 level throughout the dosing interval (mean Ctrough on Day 1 and Day 5: 2.55 μg/mL and 2.66 μg/mL, respectively). At steady state, post-dose selnoflast concentrations in sigmoid colon (5-20 μg/g) were above the IC90 . Production of IL-1β was reduced in whole blood following ex vivo stimulation with lipopolysaccharide (LPS) (in the selnoflast arm). No changes were observed in plasma IL-18 levels. There were no meaningful differences in the expression of an IL-1-related gene signature in sigmoid colon tissue, and no differences in the expression of stool biomarkers.
Conclusions: Selnoflast was safe and well-tolerated. Selnoflast 450 mg QD achieved plasma and tissue exposure predicted to maintain IL-1β IC90 over the dosing interval. However, PD biomarker results showed no robust differences between treatment arms, suggesting no major therapeutic effects are to be expected in UC. The limitations of this study are its small sample size and indirect assessment of the effect on IL-1β in tissue.
Trial registration: ISRCTN16847938.
Keywords: NLRP3 inflammasome; NLRP3 inhibitor; biomarker; inflammatory bowel disease; interleukin-1β; pharmacokinetics; phase 1b; safety; ulcerative colitis.
© 2023 F. Hoffmann-La Roche AG and The Authors. Clinical and Translational Medicine published by John Wiley & Sons Australia, Ltd on behalf of Shanghai Institute of Clinical Bioinformatics.
Conflict of interest statement
BK, LP, AN, SN, AB, SD, PG, PS, JDZ, CFC and AC were employees of F. Hoffmann‐La Roche AG Switzerland, and LB was an employee of Roche Products Ltd., UK, during the conduct of the study. JH and SB were consultants.
Figures

References
-
- Moradkhani A, Beckman LJ, Tabibian JH. Health‐related quality of life in inflammatory bowel disease: psychosocial, clinical, socioeconomic, and demographic predictors. J Crohn's Colitis. 2013;7(6):467‐473. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous