Acupuncture vs Massage for Pain in Patients Living With Advanced Cancer: The IMPACT Randomized Clinical Trial
- PMID: 37962891
- PMCID: PMC10646731
- DOI: 10.1001/jamanetworkopen.2023.42482
Acupuncture vs Massage for Pain in Patients Living With Advanced Cancer: The IMPACT Randomized Clinical Trial
Abstract
Importance: Pain is challenging for patients with advanced cancer. While recent guidelines recommend acupuncture and massage for cancer pain, their comparative effectiveness is unknown.
Objective: To compare the effects of acupuncture and massage on musculoskeletal pain among patients with advanced cancer.
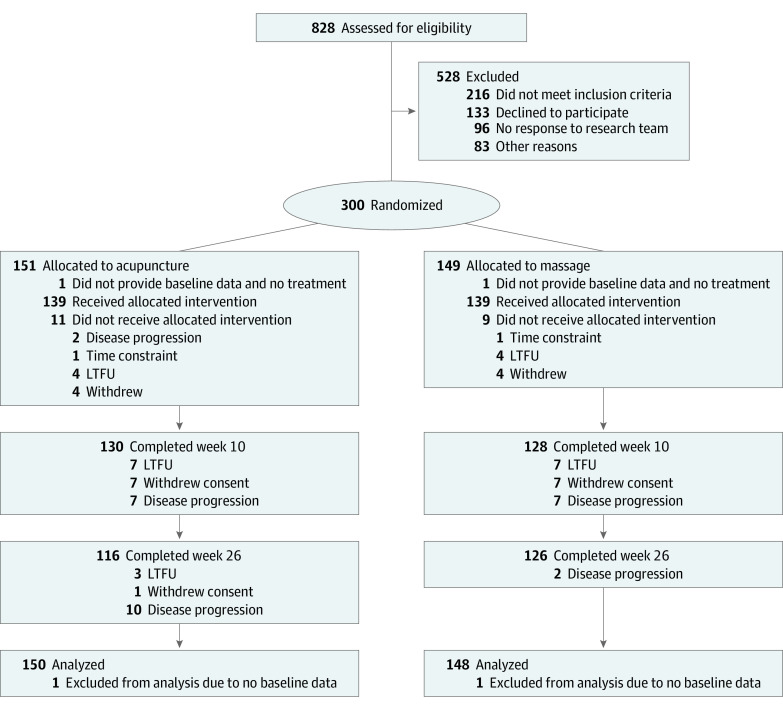
Design, setting, and participants: A multicenter pragmatic randomized clinical trial was conducted at US cancer care centers consisting of a northeastern comprehensive cancer center and a southeastern cancer institute from September 19, 2019, through February 23, 2022. The principal investigator and study statisticians were blinded to treatment assignments. The duration of follow-up was 26 weeks. Intention-to-treat analyses were performed (linear mixed models). Participants included patients with advanced cancer with moderate to severe pain and clinician-estimated life expectancy of 6 months or more. Patient recruitment strategy was multipronged (eg, patient database queries, mailings, referrals, community outreach). Eligible patients had English or Spanish as their first language, were older than 18 years, and had a Karnofsky score greater than or equal to 60 (range, 0-100; higher scores indicating less functional impairment).
Interventions: Weekly acupuncture or massage for 10 weeks with monthly booster sessions up to 26 weeks.
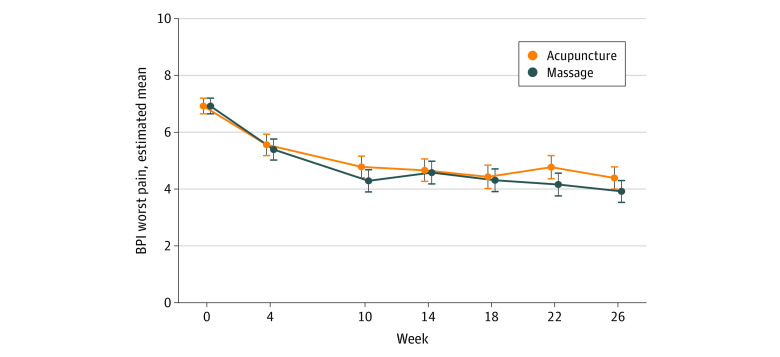
Main outcomes and measures: The primary end point was the change in worst pain intensity score from baseline to 26 weeks. The secondary outcomes included fatigue, insomnia, and quality of life. The Brief Pain Inventory (range, 0-10; higher numbers indicate worse pain intensity or interference) was used to measure the primary outcome. The secondary outcomes included fatigue, insomnia, and quality of life.
Results: A total of 298 participants were enrolled (mean [SD] age, 58.7 [14.1] years, 200 [67.1%] were women, 33 [11.1%] Black, 220 [74.1%] White, 46 [15.4%] Hispanic, and 78.5% with solid tumors). The mean (SD) baseline worst pain score was 6.9 (1.5). During 26 weeks, acupuncture reduced the worst pain score, with a mean change of -2.53 (95% CI, -2.92 to -2.15) points, and massage reduced the Brief Pain Inventory worst pain score, with a mean change of -3.01 (95% CI, -3.38 to -2.63) points; the between-group difference was not significant (-0.48; 95% CI, -0.98 to 0.03; P = .07). Both treatments also improved fatigue, insomnia, and quality of life without significant between-group differences. Adverse events were mild and included bruising (6.5% of patients receiving acupuncture) and transient soreness (15.1% patients receiving massage).
Conclusions and relevance: In this randomized clinical trial among patients with advanced cancer, both acupuncture and massage were associated with pain reduction and improved fatigue, insomnia, and quality of life over 26 weeks; however, there was no significant different between the treatments. More research is needed to evaluate how best to integrate these approaches into pain treatment to optimize symptom management for the growing population of people living with advanced cancer.
Trial registration: ClinicalTrials.gov Identifier: NCT04095234.
Conflict of interest statement
Figures