

Acinetobacter spp. bloodstream infection in hematological patients: a 10-year single-center study
- PMID: 37964192
- PMCID: PMC10648370
- DOI: 10.1186/s12879-023-08789-6
Acinetobacter spp. bloodstream infection in hematological patients: a 10-year single-center study
Abstract
Purpose: This study investigated the clinical and antimicrobial characteristics of Acinetobacter spp. bloodstream infection (BSI) in hematological patients. Risk factors for 30-day mortality and carbapenem-resistant Acinetobacter spp. (CRA) BSI acquisition were also identified.
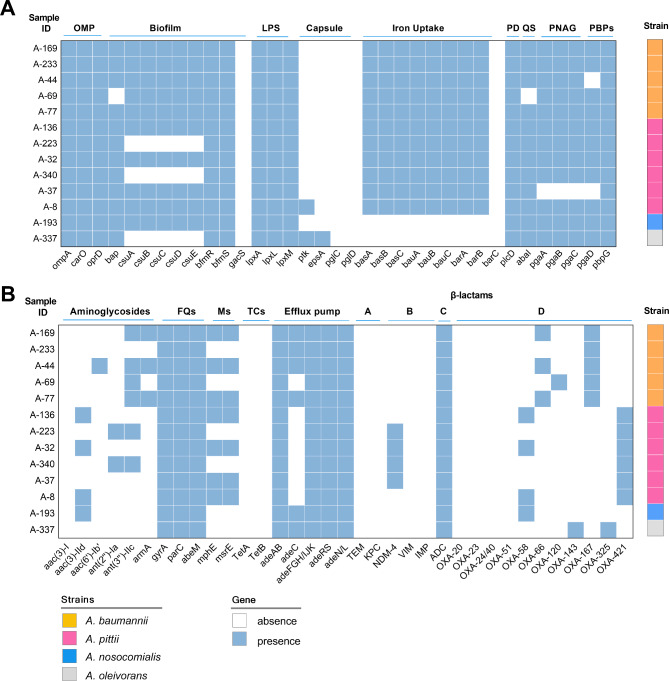
Methods: We reviewed forty hematological patients with Acinetobacter spp. BSI in a large Chinese blood disease hospital between 2013 and 2022. The remaining CRA isolates were subjected to whole-genome sequencing.
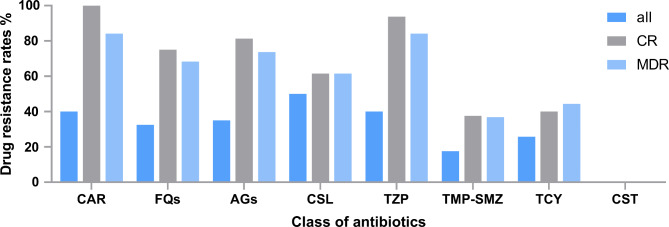
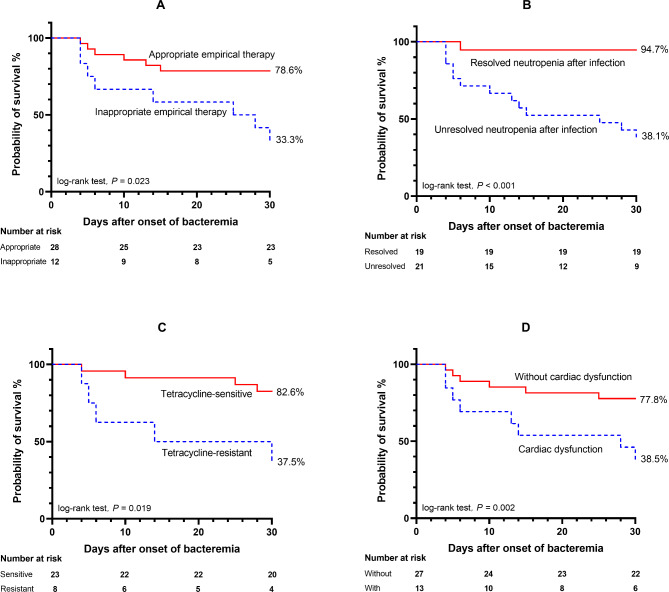
Results: The 30-day mortality rate was high at 35%. Hematological patients with Acinetobacter spp. BSI often presented with severe conditions and co-infections at multiple sites. All strains were colistin-susceptible and 40.0% were CR. Multivariate analysis identified several risk factors associated with CRA BSI acquisition, including previous exposure to carbapenems within 30 days and CRA colonization. Very severe aplastic anaemia, tetracycline-resistant Acinetobacter spp. BSI, and unresolved neutropenia after infection were closely associated with 30-day mortality. Non-survivors often presented with higher median PCT and CRP levels and severe complications, such as intracranial infection, cardiac dysfunction, respiratory failure, and severe sepsis or septic shock. Our study also identified inappropriate empirical antibiotic therapy as an independent predictor of 30-day mortality (OR: 11.234, 95% CI: 1.261-20.086, P = 0.030). This study was the first to report A. oleivorans as a human pathogen, and to identify its unique oxacillinase, OXA-325.
Conclusion: An environment-originated non-pathogenic species can become pathogenic when the body's immunity is compromised. Our results also highlighted the importance of improving neutropenia after infection, treating severe organ dysfunction, and administering appropriate empirical antibiotic therapy to reduce mortality in this patient population.
Keywords: Acinetobacter; Bloodstream Infection; Outcome; Risk factors; Treatment.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Strong Homology Between Colonizing and Bloodstream Carbapenem-Resistant Acinetobacter Spp.: Implications for Empiric Antibiotic Therapy in Hematological Patients.Infect Drug Resist. 2024 May 9;17:1827-1838. doi: 10.2147/IDR.S458427. eCollection 2024. Infect Drug Resist. 2024. PMID: 38741942 Free PMC article.
-
Epidemiology of and risk factors for Acinetobacter species bloodstream infection in children.Pediatr Infect Dis J. 2007 Oct;26(10):920-6. doi: 10.1097/INF.0b013e3180684310. Pediatr Infect Dis J. 2007. PMID: 17901798
-
Outcomes and appropriateness of management of nosocomial Acinetobacter bloodstream infections at a teaching hospital in northeastern Malaysia.Southeast Asian J Trop Med Public Health. 2009 Jan;40(1):140-7. Southeast Asian J Trop Med Public Health. 2009. PMID: 19323046
-
[Pathogenic role of Acinetobacter spp during HIV infection].Infez Med. 2001 Mar;9(1):43-51. Infez Med. 2001. PMID: 12082349 Review. Italian.
-
Rates, predictors and mortality of community-onset bloodstream infections due to Pseudomonas aeruginosa: systematic review and meta-analysis.Clin Microbiol Infect. 2019 Aug;25(8):964-970. doi: 10.1016/j.cmi.2019.04.005. Epub 2019 Apr 14. Clin Microbiol Infect. 2019. PMID: 30995530
Cited by
-
Adult acute leukemia patients with gram-negative bacteria bloodstream infection: Risk factors and outcomes of antibiotic-resistant bacteria.Ann Hematol. 2024 Oct;103(10):4021-4031. doi: 10.1007/s00277-024-05866-x. Epub 2024 Jul 3. Ann Hematol. 2024. PMID: 38958702 Free PMC article.
-
Bloodstream infection by Lactobacillus rhamnosus in a haematology patient: why metagenomics can make the difference.Gut Pathog. 2025 Jun 21;17(1):47. doi: 10.1186/s13099-025-00722-3. Gut Pathog. 2025. PMID: 40544256 Free PMC article.
-
Strong Homology Between Colonizing and Bloodstream Carbapenem-Resistant Acinetobacter Spp.: Implications for Empiric Antibiotic Therapy in Hematological Patients.Infect Drug Resist. 2024 May 9;17:1827-1838. doi: 10.2147/IDR.S458427. eCollection 2024. Infect Drug Resist. 2024. PMID: 38741942 Free PMC article.
-
Rhino-orbito-cerebral mucormycosis after allogeneic hematopoietic stem cell transplantation for very severe aplastic anemia in a child: a case report.Front Pediatr. 2025 Apr 14;13:1529656. doi: 10.3389/fped.2025.1529656. eCollection 2025. Front Pediatr. 2025. PMID: 40297559 Free PMC article.
References
-
- Balkhair A, Al-Muharrmi Z, Al’adawi B, et al. Prevalence and 30-day all-cause mortality of carbapenem-and colistin-resistant bacteraemia caused by Acinetobacter baumannii, Pseudomonas aeruginosa, and Klebsiella pneumoniae: description of a decade-long trend[J] Int J Infect Dis. 2019;85:10–5. doi: 10.1016/j.ijid.2019.05.004. - DOI - PubMed
-
- Freire MP, De Oliveira Garcia D, Garcia CP, et al. Bloodstream Infection caused by extensively drug-resistant Acinetobacter baumannii in cancer patients: high mortality associated with delayed treatment rather than with the degree of neutropenia[J] Clin Microbiol Infect. 2016;22(4):352–8. doi: 10.1016/j.cmi.2015.12.010. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 2021-I2M-1-017/the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences
- 2021-I2M-1-017/the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences
- 2021-I2M-1-017/the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences
- 2021-I2M-1-017/the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences
- 21JCZDJC01170/the Tianjin Municipal Science and Technology Commission Grant
- 21JCZDJC01170/the Tianjin Municipal Science and Technology Commission Grant
- 21JCZDJC01170/the Tianjin Municipal Science and Technology Commission Grant
- 21JCZDJC01170/the Tianjin Municipal Science and Technology Commission Grant
- 22HHXBSS00036/Haihe Laboratory of Cell Ecosystem Innovation Fund
- 22HHXBSS00036/Haihe Laboratory of Cell Ecosystem Innovation Fund
- 22HHXBSS00036/Haihe Laboratory of Cell Ecosystem Innovation Fund
- 22HHXBSS00036/Haihe Laboratory of Cell Ecosystem Innovation Fund
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
