

Personalized surveillance and aftercare for non-metastasized breast cancer: the NABOR study protocol of a multiple interrupted time series design
- PMID: 37964214
- PMCID: PMC10647159
- DOI: 10.1186/s12885-023-11504-y
Personalized surveillance and aftercare for non-metastasized breast cancer: the NABOR study protocol of a multiple interrupted time series design
Abstract
Background: Follow-up of curatively treated primary breast cancer patients consists of surveillance and aftercare and is currently mostly the same for all patients. A more personalized approach, based on patients' individual risk of recurrence and personal needs and preferences, may reduce patient burden and reduce (healthcare) costs. The NABOR study will examine the (cost-)effectiveness of personalized surveillance (PSP) and personalized aftercare plans (PAP) on patient-reported cancer worry, self-rated and overall quality of life and (cost-)effectiveness.
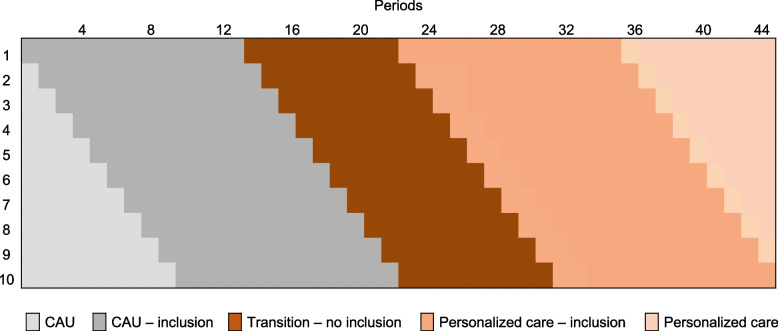
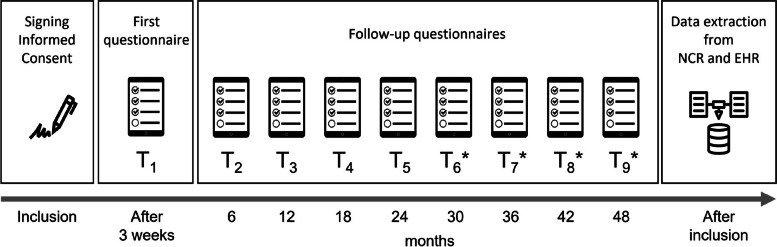
Methods: A prospective multicenter multiple interrupted time series (MITs) design is being used. In this design, 10 participating hospitals will be observed for a period of eighteen months, while they -stepwise- will transit from care as usual to PSPs and PAPs. The PSP contains decisions on the surveillance trajectory based on individual risks and needs, assessed with the 'Breast Cancer Surveillance Decision Aid' including the INFLUENCE prediction tool. The PAP contains decisions on the aftercare trajectory based on individual needs and preferences and available care resources, which decision-making is supported by a patient decision aid. Patients are non-metastasized female primary breast cancer patients (N = 1040) who are curatively treated and start follow-up care. Patient reported outcomes will be measured at five points in time during two years of follow-up care (starting about one year after treatment and every six months thereafter). In addition, data on diagnostics and hospital visits from patients' Electronical Health Records (EHR) will be gathered. Primary outcomes are patient-reported cancer worry (Cancer Worry Scale) and overall quality of life (as assessed with EQ-VAS score). Secondary outcomes include health care costs and resource use, health-related quality of life (as measured with EQ5D-5L/SF-12/EORTC-QLQ-C30), risk perception, shared decision-making, patient satisfaction, societal participation, and cost-effectiveness. Next, the uptake and appreciation of personalized plans and patients' experiences of their decision-making process will be evaluated.
Discussion: This study will contribute to insight in the (cost-)effectiveness of personalized follow-up care and contributes to development of uniform evidence-based guidelines, stimulating sustainable implementation of personalized surveillance and aftercare plans.
Trial registration: Study sponsor: ZonMw. Retrospectively registered at ClinicalTrials.gov (2023), ID: NCT05975437.
Keywords: Aftercare; Breast cancer; Decision-making; Personalized follow-up; Risk of recurrence; Surveillance.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- NKR. NKR Cijfers. 2021. https://iknl.nl/nkr-cijfers. Accessed 20 Jul 2023.
-
- NABON. Borstkanker. 2017. https://richtlijnendatabase.nl/richtlijn/borstkanker/nazorg_en_nacontrol.... Accessed 7 Jul 2022.
-
- van Maaren MC, Strobbe LJA, Smidt ML, Moossdorff M, Poortmans PMP, Siesling S. Ten-year conditional recurrence risks and overall and relative survival for breast cancer patients in the Netherlands: Taking account of event-free years. Eur J Cancer. 2018;102:82–94. doi: 10.1016/j.ejca.2018.07.124. - DOI - PubMed
-
- Witteveen A, Vliegen IMH, Sonke GS, Klaase JM, IJzerman MJ, Siesling S. Personalisation of breast cancer follow-up: a time-dependent prognostic nomogram for the estimation of annual risk of locoregional recurrence in early breast cancer patients. Breast Cancer Res Treat. 2015;152(3):627–36. doi: 10.1007/s10549-015-3490-4. - DOI - PMC - PubMed
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
