

Evaluating residual tumor after neoadjuvant chemotherapy for muscle-invasive urothelial bladder cancer: diagnostic performance and outcomes using biparametric vs. multiparametric MRI
- PMID: 37964386
- PMCID: PMC10644594
- DOI: 10.1186/s40644-023-00632-0
Evaluating residual tumor after neoadjuvant chemotherapy for muscle-invasive urothelial bladder cancer: diagnostic performance and outcomes using biparametric vs. multiparametric MRI
Abstract
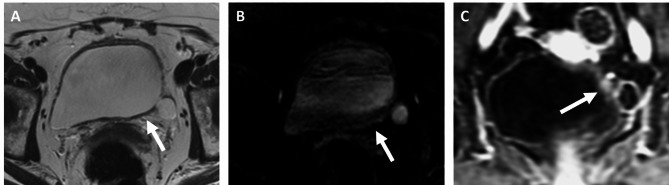
Background: Neoadjuvant chemotherapy (NAC) before radical cystectomy is standard of care in patients with muscle-invasive bladder cancer (MIBC). Response assessment after NAC is important but suboptimal using CT. We assessed MRI without vs. with intravenous contrast (biparametric [BP] vs. multiparametric [MP]) for identifying residual disease on cystectomy and explored its prognostic role.
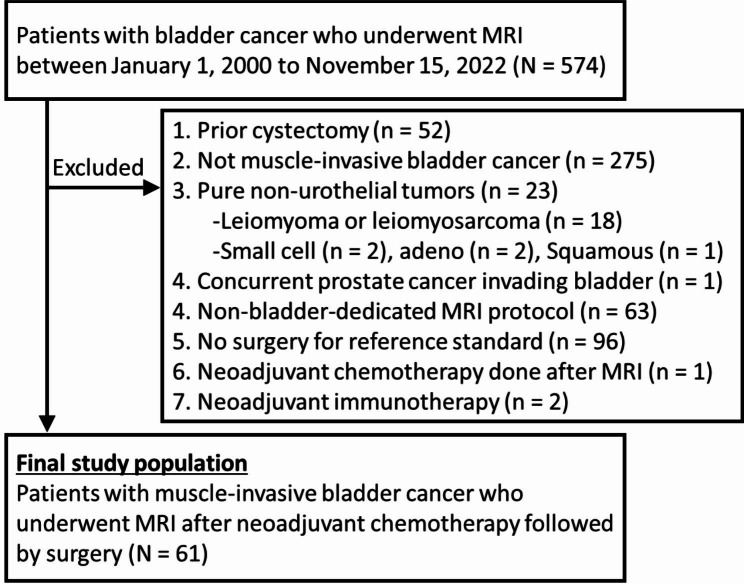
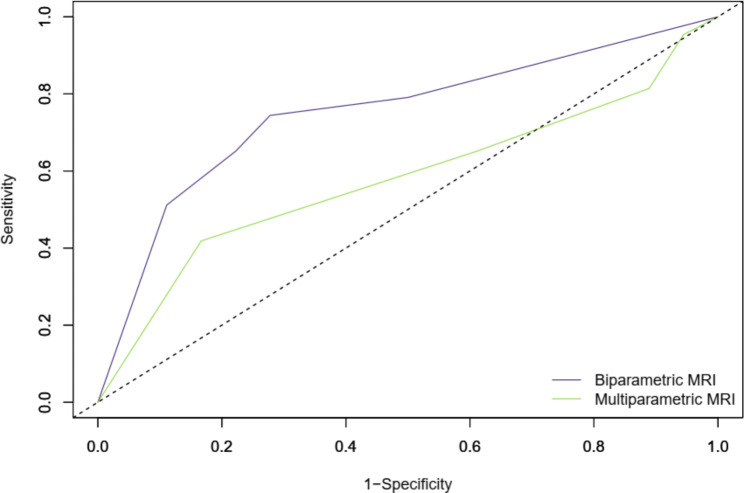
Methods: Consecutive MIBC patients that underwent NAC, MRI, and cystectomy between January 2000-November 2022 were identified. Two radiologists reviewed BP-MRI (T2 + DWI) and MP-MRI (T2 + DWI + DCE) for residual tumor. Diagnostic performances were compared using receiver operating characteristic curve analysis. Kaplan-Meier curves and Cox proportional-hazards models were used to evaluate association with disease-free survival (DFS).
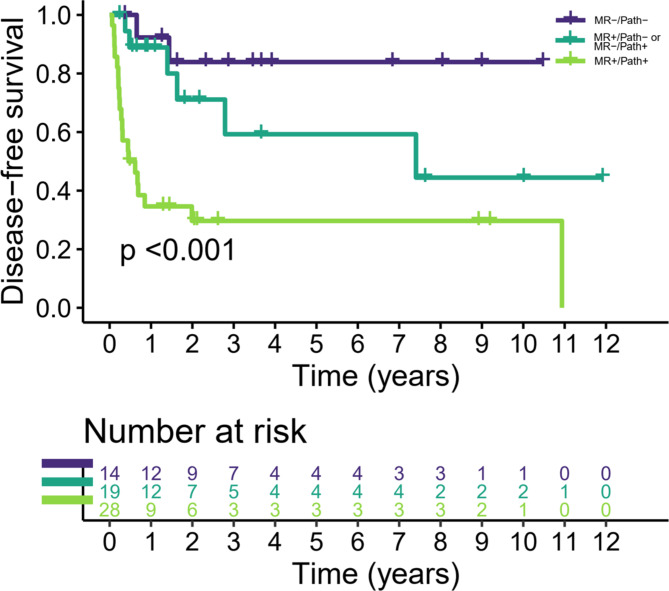
Results: 61 patients (36 men and 25 women; median age 65 years, interquartile range 59-72) were included. After NAC, no residual disease was detected on pathology in 19 (31.1%) patients. BP-MRI was more accurate than MP-MRI for detecting residual disease after NAC: area under the curve = 0.75 (95% confidence interval (CI), 0.62-0.85) vs. 0.58 (95% CI, 0.45-0.70; p = 0.043). Sensitivity were identical (65.1%; 95% CI, 49.1-79.0) but specificity was higher in BP-MRI compared with MP-MRI for determining residual disease: 77.8% (95% CI, 52.4-93.6) vs. 38.9% (95% CI, 17.3-64.3), respectively. Positive BP-MRI and residual disease on pathology were both associated with worse DFS: hazard ratio (HR) = 4.01 (95% CI, 1.70-9.46; p = 0.002) and HR = 5.13 (95% CI, 2.66-17.13; p = 0.008), respectively. Concordance between MRI and pathology results was significantly associated with DFS. Concordant positive (MRI+/pathology+) patients showed worse DFS than concordant negative (MRI-/pathology-) patients (HR = 8.75, 95% CI, 2.02-37.82; p = 0.004) and compared to the discordant group (MRI+/pathology- or MRI-/pathology+) with HR = 3.48 (95% CI, 1.39-8.71; p = 0.014).
Conclusion: BP-MRI was more accurate than MP-MRI for identifying residual disease after NAC. A negative BP-MRI was associated with better outcomes, providing complementary information to pathological assessment of cystectomy specimens.
Keywords: Biparametric; Cystectomy; Magnetic resonance imaging; Multiparametric; Muscle-invasive bladder cancer; Neoadjuvant chemotherapy; Prognosis; Response assessment; Survival; Urothelial.
© 2023. The Author(s).
Conflict of interest statement
MYT has equity interests at Clovis Oncology and provides services to Janssen Global Services, LLC. ACG is a consultant to Medtronics for provision of Services for which he does not receive compensation. The other authors do not have anything to disclose. Aforementioned entities were not involved in the design, conduct, or manuscript writing of this study.
Figures
References
-
- International Collaboration of Trialists, Medical Research Council Advanced Bladder Cancer Working Party (now the National Cancer Research Institute Bladder Cancer Clinical Studies Group), European Organisation for Research and Treatment of Cancer Genito-Urinary Tract Cancer Group, Australian Bladder Cancer Study Group, National Cancer Institute of Canada Clinical Trials Group. Finnbladder, et al. International phase III trial assessing neoadjuvant cisplatin, methotrexate, and vinblastine chemotherapy for muscle-invasive Bladder cancer: long-term results of the BA06 30894 trial. J Clin Oncol off J Am Soc Clin Oncol. 2011;29(16):2171–7. doi: 10.1200/JCO.2010.32.3139. - DOI - PMC - PubMed
-
- Choueiri TK, Jacobus S, Bellmunt J, Qu A, Appleman LJ, Tretter C, et al. Neoadjuvant dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin with pegfilgrastim support in muscle-invasive urothelial cancer: pathologic, radiologic, and biomarker correlates. J Clin Oncol off J Am Soc Clin Oncol. 2014;32(18):1889–94. doi: 10.1200/JCO.2013.52.4785. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
