

Reverse or Ulnar-Sided, Greater Arc Perilunate Injury: Case Report and Systematic Review of Literature
- PMID: 37964486
- PMCID: PMC11833847
- DOI: 10.1177/15589447231211605
Reverse or Ulnar-Sided, Greater Arc Perilunate Injury: Case Report and Systematic Review of Literature
Abstract
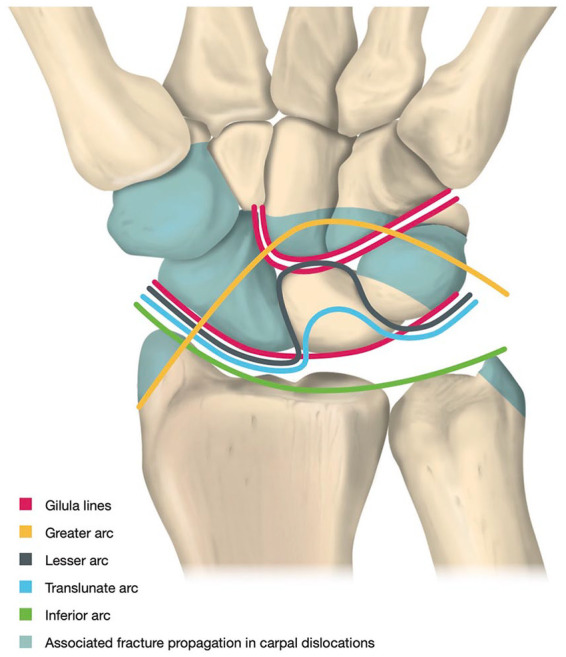
Background: Perilunate injuries of carpal bones are uncommon, high-energy injuries that necessitate early diagnosis and appropriate management to prevent progressive carpal instability and posttraumatic osteoarthritis. A much more uncommon mechanism that starts from the lunotriquetral ligament and proceeds radially in an opposite direction than the classic mechanism may cause a reverse or ulnar-sided perilunate dislocation (PLD). The purposes were: (1) to present an uncommon case of greater arc reverse (ulnar-sided) perilunate fracture-dislocation (REPLFD); and (2) to conduct a systematic review (SR) to evaluate the current evidence on reverse perilunate injuries (REPLIs).
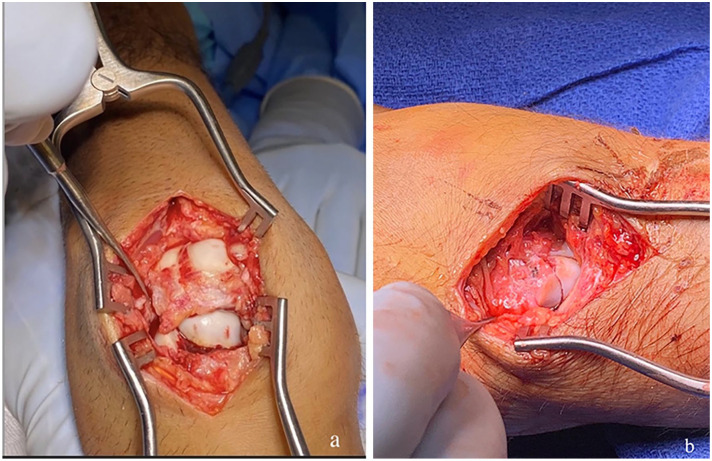
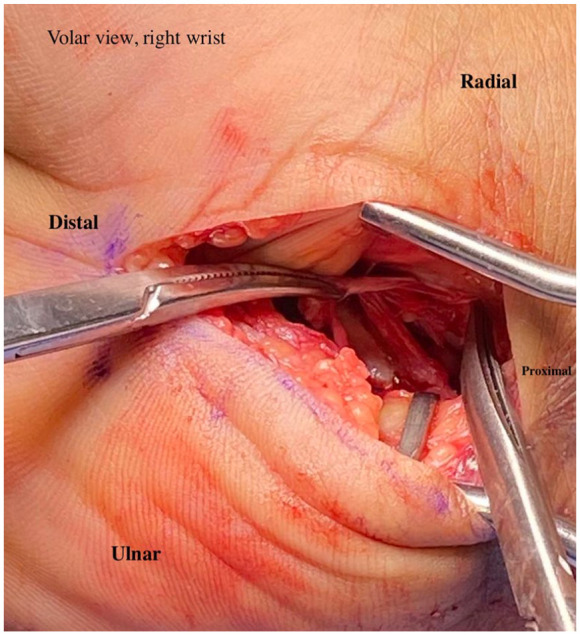
Methods: A novel pattern of injury of REPLFD with fractures of the ulnar styloid, triquetrum, and capitate is presented. A SR was conducted with primary outcome measures of the type of injury (pathoanatomy of lesions) and pathomechanics. Secondary outcome measures were choice of surgery and outcome on follow-up.
Results: The Murad's tool and modified Coleman Methodology Score revealed poor methodological quality of the available literature on REPLI. Evidence is lacking in the mechanism of injury and treatment of REPLI, especially regarding REPLFD.
Conclusions: The SR revealed poor methodological quality of the available literature and exposes that not all PLDs can be explained by the current existing pathomechanical injury classifications. However, following the management principles of perilunate injuries, REPLI tends to have good functional results with no major complications.
Level of evidence: Level V.
Keywords: carpal instability; perilunate fracture-dislocation; reverse perilunate; ulnar-sided perilunate; wrist dislocation.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures



References
-
- Forli A, Courvoisier A, Wimsey S, et al.. Perilunate dislocations and transscaphoid perilunate fracture-dislocations: a retrospective study with minimum ten-year follow-up. J Hand Surg Am. 2010;35(1):62-68. - PubMed
-
- Herzberg G, Comtet JJ, Linscheid RL, et al.. Perilunate dislocations and fracture-dislocations: a multicenter study. J Hand Surg Am. 1993;18(5):768-779. - PubMed
-
- Herzberg G. Perilunate and axial carpal dislocations and fracture-dislocations. J Hand Surg Am. 2008;33(9):1659-1668. - PubMed
-
- Mayfield JK, Johnson RP, Kilcoyne RK. Carpal dislocations: pathomechanics and progressive perilunar instability. J Hand Surg Am. 1980;5(3):226-241. - PubMed
-
- Johnson RP. The acutely injured wrist and its residuals. Clin Orthop Relat Res. 1980;149:33-44. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
