

Posthospital Multidisciplinary Care for AKI Survivors: A Feasibility Pilot
- PMID: 37964784
- PMCID: PMC10641567
- DOI: 10.1016/j.xkme.2023.100734
Posthospital Multidisciplinary Care for AKI Survivors: A Feasibility Pilot
Abstract
Rationale & objective: Innovative models are needed to address significant gaps in kidney care follow-up for acute kidney injury (AKI) survivors.
Study design: This quasi-experimental pilot study reports the feasibility of the AKI in Care Transitions (ACT) program, a multidisciplinary approach to AKI survivor care based in the primary care setting.
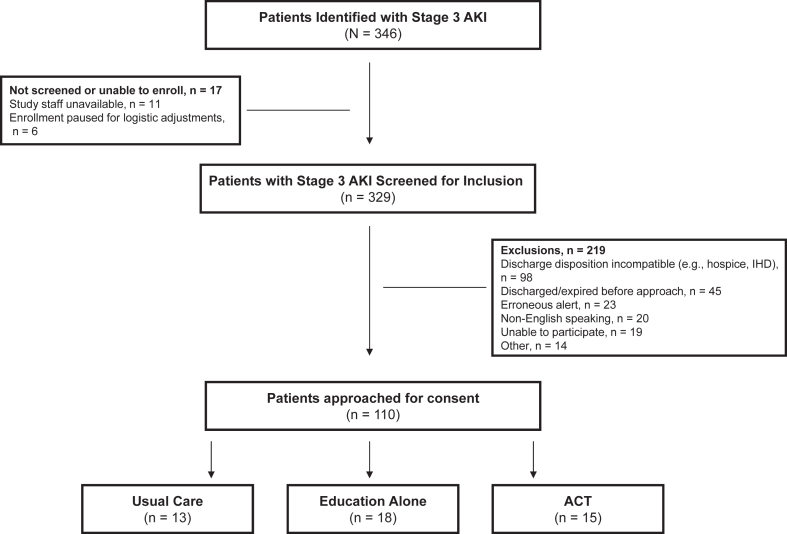
Setting & participants: The study included consenting adults with stage 3 AKI discharged home without dialysis.
Interventions: The ACT intervention included predischarge education from nurses and coordinated postdischarge follow-up with a primary care provider and pharmacist within 14 days. ACT was implemented in phases (Usual Care, Education, ACT).
Outcomes: The primary outcome was feasibility. Secondary outcomes included process and clinical outcomes.
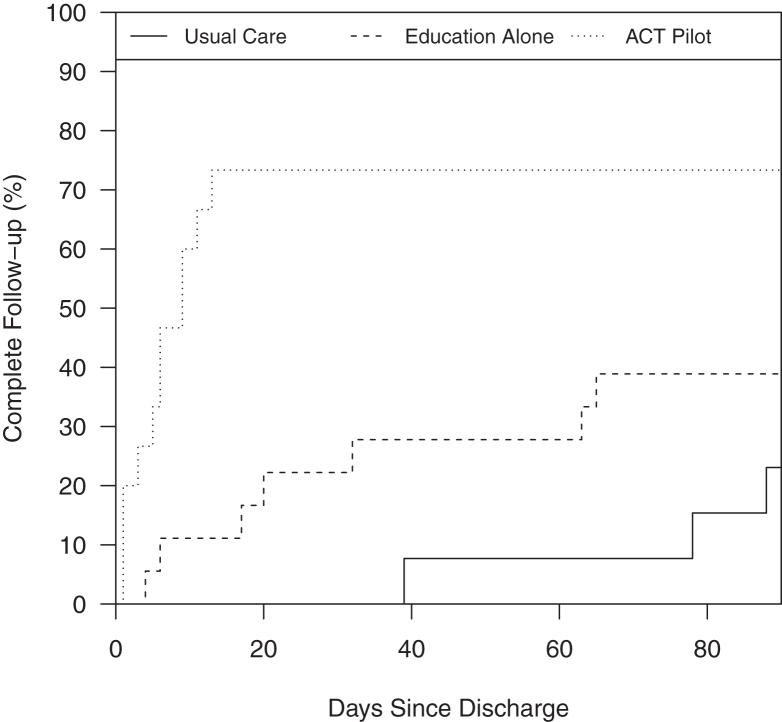
Results: In total, 46 of 110 eligible adults were enrolled. Education occurred in 18/18 and 14/15 participants in the Education and ACT groups, respectively. 30-day urine protein evaluation occurred in 15%, 28%, and 87% of the Usual Care, Education, and ACT groups, respectively (P < 0.001). Cumulative incidence of provider (primary care or nephrologist) and laboratory follow-up at 14 and 30 days was different across groups (14 days: Usual care 0%, Education 11%, ACT 73% [P < 0.01]; 30 days: 0%, 22%, and 73% [P < 0.01]). 30-day readmission rates were 23%, 44%, and 13% in the Usual Care, Education, and ACT groups, respectively (P = 0.13).
Limitations: Patients were not randomly assigned to treatment groups. The sample size limited the ability to detect some differences or perform multivariable analysis.
Conclusions: This study demonstrated the feasibility of multidisciplinary AKI survivor follow-up beginning in primary care. We observed a higher cumulative incidence of laboratory and provider follow-up in ACT participants.
Trial registration: ClinicalTrials.gov (NCT04505891).
Plain-language summary: Abrupt loss of kidney function in hospitalized patients, acute kidney injury (AKI), increases the chances of long-term kidney disease and a worse health care experience for patients. One out of 3 people who experience AKI do not get the follow-up kidney care they need. We performed a pilot study to test whether a program that facilitates structured AKI follow-up in primary care called the AKI in Care Transitions (ACT) program was possible. ACT brings together the unique expertise of nurses, doctors, and pharmacists to look at the patient's kidney health plan from all angles. The study found that the ACT program was possible and led to more complete kidney care follow-up after discharge than the normal approach to care.
Keywords: Acute kidney injury; acute kidney injury; care transitions; chronic kidney disease; patient care team; pharmacist; primary care.
© 2023 The Authors.
Figures

References
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
