

Symptomatic periesophageal vagal nerve injury by different energy sources during atrial fibrillation ablation
- PMID: 37965084
- PMCID: PMC10642562
- DOI: 10.3389/fcvm.2023.1278603
Symptomatic periesophageal vagal nerve injury by different energy sources during atrial fibrillation ablation
Abstract
Background: Symptomatic gastric hypomotility (SGH) is a rare but major complication of atrial fibrillation (AF) ablation, but data on this are scarce.
Objective: We compared the clinical course of SGH occurring with different energy sources.
Methods: This multicenter study retrospectively collected the characteristics and clinical outcomes of patients with SGH after AF ablation.
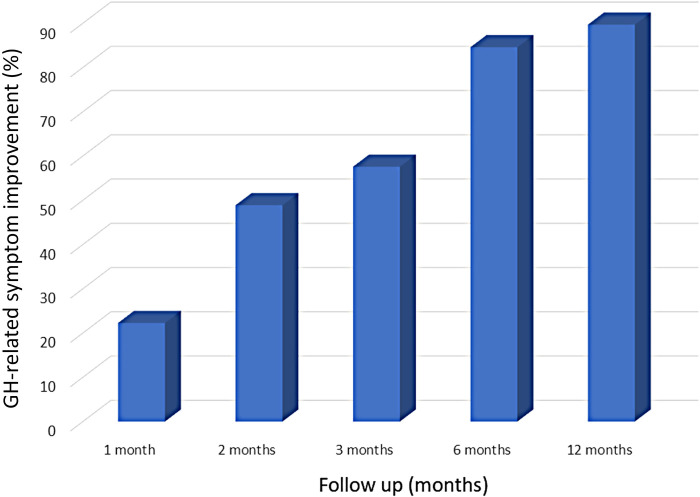
Results: The data of 93 patients (67.0 ± 11.2 years, 68 men, 52 paroxysmal AF) with SGH after AF ablation were collected from 23 cardiovascular centers. Left atrial (LA) ablation sets included pulmonary vein isolation (PVI) alone, a PVI plus a roof-line, and an LA posterior wall isolation in 42 (45.2%), 11 (11.8%), and 40 (43.0%) patients, respectively. LA ablation was performed by radiofrequency ablation, cryoballoon ablation, or both in 38 (40.8%), 38 (40.8%), and 17 (18.3%) patients, respectively. SGH diagnoses were confirmed at 2 (1-4) days post-procedure, and 28 (30.1%) patients required re-hospitalizations. Fasting was required in 81 (92.0%) patients for 4 (2.5-5) days; the total hospitalization duration was 11 [7-19.8] days. After conservative treatment, symptoms disappeared in 22.3% of patients at 1 month, 48.9% at 2 months, 57.6% at 3 months, 84.6% at 6 months, and 89.7% at 12 months, however, one patient required surgery after radiofrequency ablation. Symptoms persisted for >1-year post-procedure in 7 patients. The outcomes were similar regardless of the energy source and LA lesion set.
Conclusions: The clinical course of SGH was similar regardless of the energy source. The diagnosis was often delayed, and most recovered within 6 months, yet could persist for over 1 year in 10%.
Keywords: atrial fibrillation; catheter ablation; complication; gastric hypomotility; pulmonary vein isolation; vagal nerve injury.
© 2023 Miyazaki, Kobori, Jo, Keida, Yoshitani, Mukai, Sagawa, Asakawa, Sato, Yamao, Horie, Manita, Fukaya, Hayashi, Tanimoto, Iwayama, Chiba, Sato, Sekiguchi, Sugiura, Iwai, Isonaga, Miwa, Kato, Inaba, Hirota, Nagata, Ono, Hachiya, Yamauchi, Goya, Nitta, Tada and Sasano.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
References
-
- Kuwahara T, Takahashi A, Takahashi Y, Kobori A, Miyazaki S, Takei A, et al. Clinical characteristics and management of periesophageal vagal nerve injury complicating left atrial ablation of atrial fibrillation: lessons from eleven cases. J Cardiovasc Electrophysiol. (2013) 24:847–51. 10.1111/jce.12130 - DOI - PubMed
LinkOut - more resources
Full Text Sources