

Noninvasive diagnosis of secondary infections in COVID-19 by sequencing of plasma microbial cell-free DNA
- PMID: 37965142
- PMCID: PMC10641743
- DOI: 10.1016/j.isci.2023.108093
Noninvasive diagnosis of secondary infections in COVID-19 by sequencing of plasma microbial cell-free DNA
Abstract
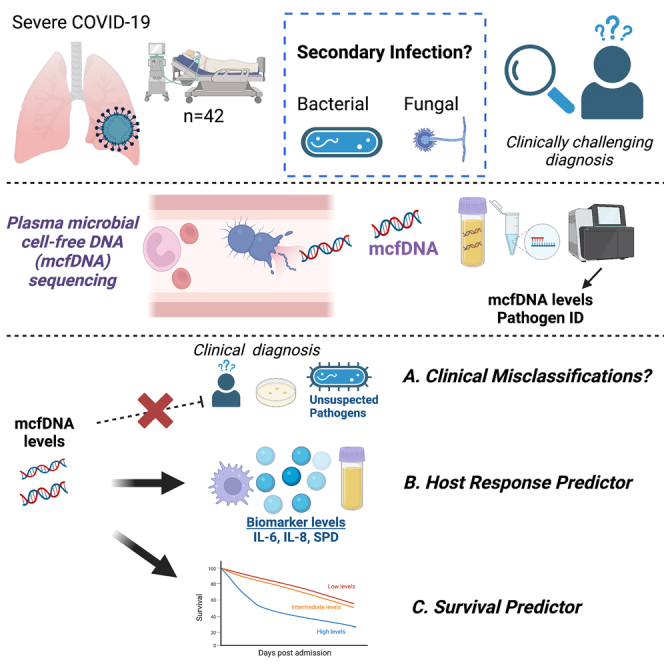
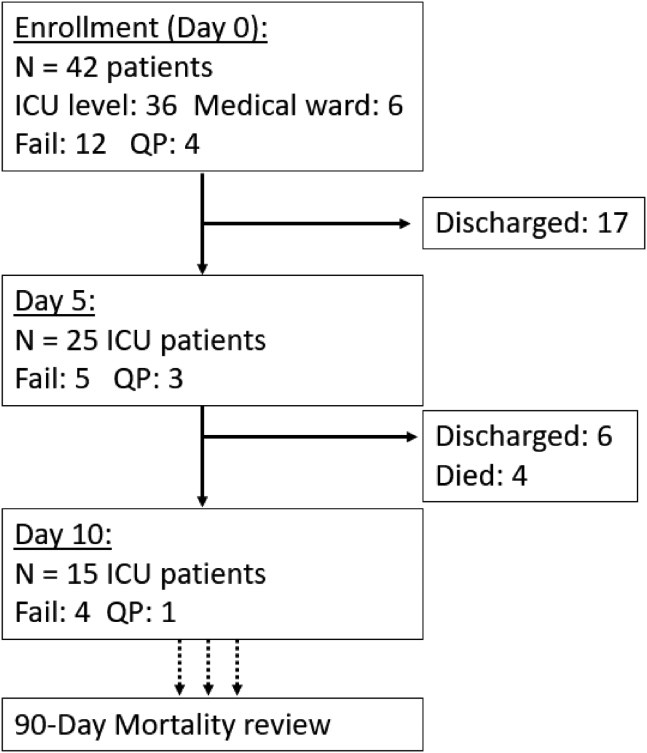
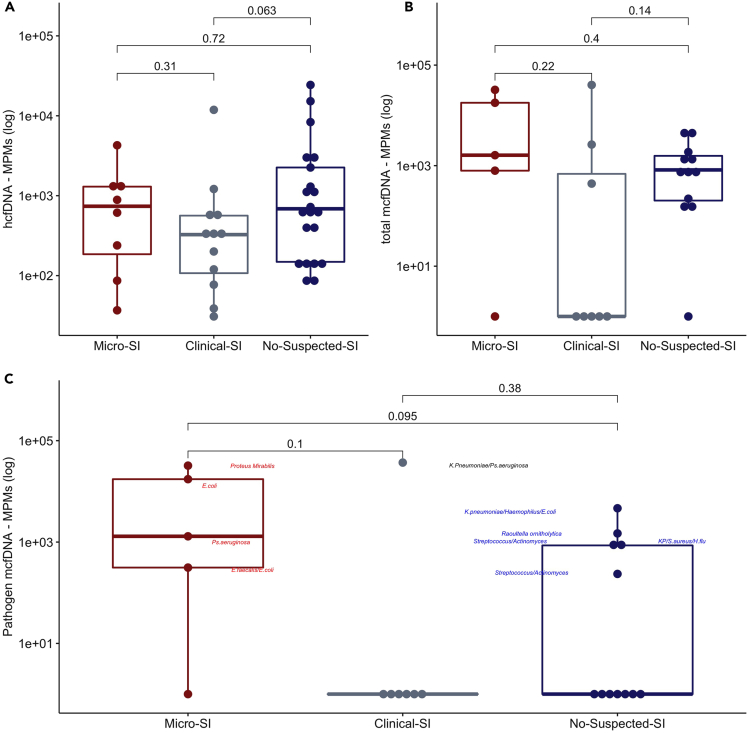
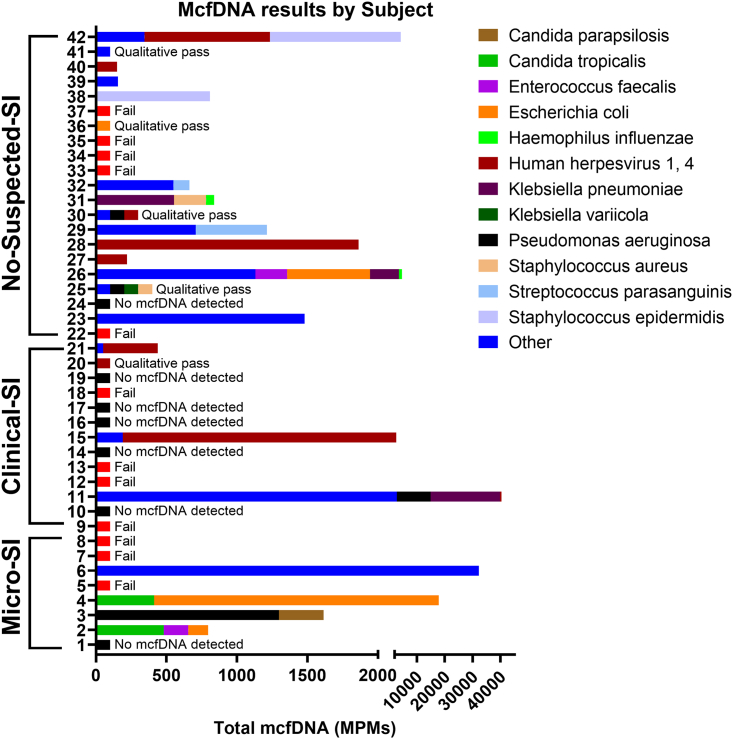
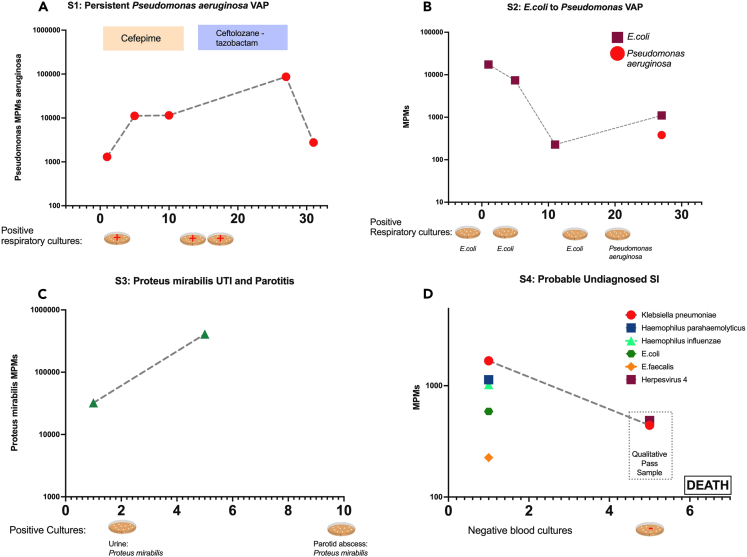
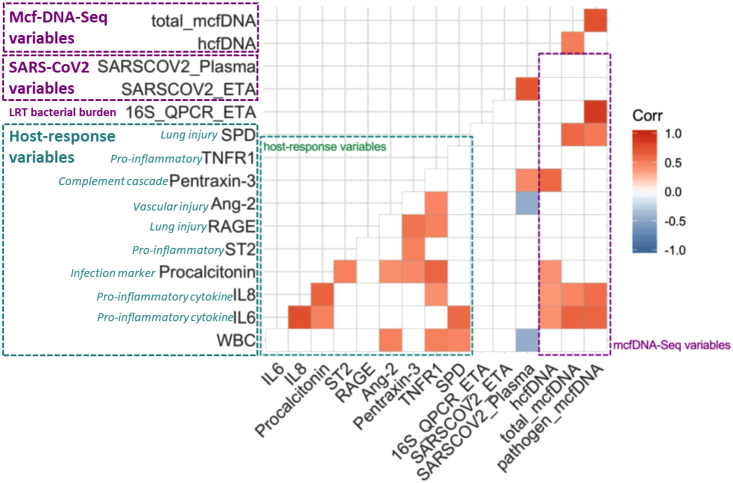
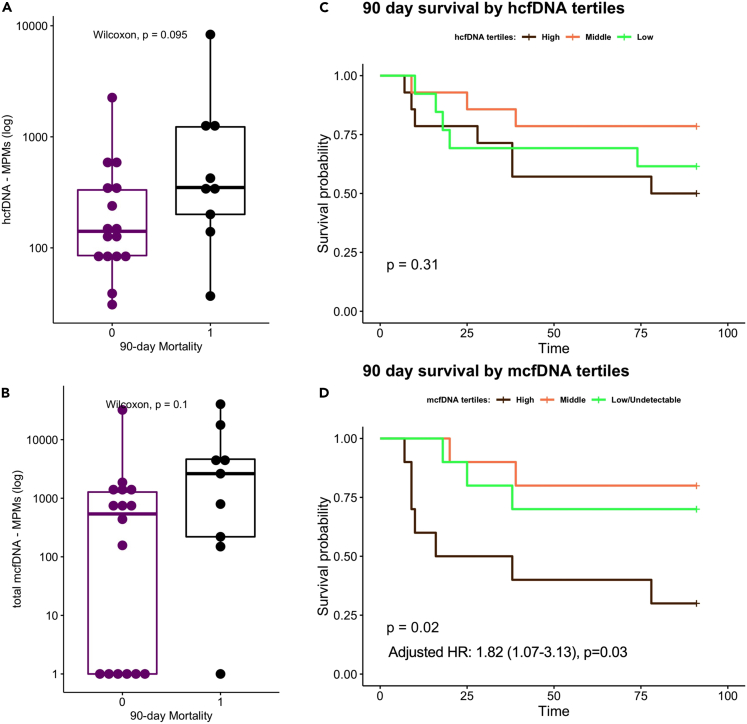
Secondary infection (SI) diagnosis in severe COVID-19 remains challenging. We correlated metagenomic sequencing of plasma microbial cell-free DNA (mcfDNA-Seq) with clinical SI assessment, immune response, and outcomes. We classified 42 COVID-19 inpatients as microbiologically confirmed-SI (Micro-SI, n = 8), clinically diagnosed-SI (Clinical-SI, n = 13, i.e., empiric antimicrobials), or no-clinical-suspicion-for-SI (No-Suspected-SI, n = 21). McfDNA-Seq was successful in 73% of samples. McfDNA detection was higher in Micro-SI (94%) compared to Clinical-SI (57%, p = 0.03), and unexpectedly high in No-Suspected-SI (83%), similar to Micro-SI. We detected culture-concordant mcfDNA species in 81% of Micro-SI samples. McfDNA correlated with LRT 16S rRNA bacterial burden (r = 0.74, p = 0.02), and biomarkers (white blood cell count, IL-6, IL-8, SPD, all p < 0.05). McfDNA levels were predictive of worse 90-day survival (hazard ratio 1.30 [1.02-1.64] for each log10 mcfDNA, p = 0.03). High mcfDNA levels in COVID-19 patients without clinical SI suspicion may suggest SI under-diagnosis. McfDNA-Seq offers a non-invasive diagnostic tool for pathogen identification, with prognostic value on clinical outcomes.
Keywords: Classification description immunology; Sequence analysis; Virology.
© 2023 The Authors.
Conflict of interest statement
Drs. Duttagupta and Ahmed were employed by Karius, Inc at the time of the study but are no longer employed by Karius, Inc. Drs. Kitsios and Haidar have received research funding from Karius, Inc. Drs. Kitsios and Morris have received research funding from Pfizer, Inc. Dr. Haidar serves on the Karius, Inc scientific advisory board. Dr. Mellors is a consultant to AlloVir, Infectious Disease Connect, Inc., and Gilead Sciences, Inc., has received research funding from Gilead Sciences, Inc. to the University of Pittsburgh, receives compensation from Abound Bio, Inc. (unrelated to the current work) and holds shares options in Galapogos, Infectious Disease Connect, Inc., and MingMed Biotechnology Co. Ltd. (unrelated to the current work). Dr. McVerry has received research funding from Bayer Pharmaceuticals, Inc. and consulting fees from Boehringer Ingelheim, both unrelated to this work.
Figures
References
-
- Zhou F., Yu T., Du R., Fan G., Liu Y., Liu Z., Xiang J., Wang Y., Song B., Gu X., et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054–1062. doi: 10.1016/s0140-6736(20)30566-3. - DOI - PMC - PubMed
-
- Rouzé A., Martin-Loeches I., Povoa P., Makris D., Artigas A., Bouchereau M., Lambiotte F., Metzelard M., Cuchet P., Boulle Geronimi C., et al. Relationship between SARS-CoV-2 infection and the incidence of ventilator-associated lower respiratory tract infections: a European multicenter cohort study. Intensive Care Med. 2021;47:188–198. doi: 10.1007/s00134-020-06323-9. - DOI - PMC - PubMed
-
- Pickens C.O., Gao C.A., Cuttica M.J., Smith S.B., Pesce L.L., Grant R.A., Kang M., Morales-Nebreda L., Bavishi A.A., Arnold J.M., et al. Bacterial Superinfection Pneumonia in Patients Mechanically Ventilated for COVID-19 Pneumonia. Am. J. Respir. Crit. Care Med. 2021;204:921–932. doi: 10.1164/rccm.202106-1354OC. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
