

Multimodal Analysis of Secondary Cerebellar Alterations After Pediatric Traumatic Brain Injury
- PMID: 37966838
- PMCID: PMC10652147
- DOI: 10.1001/jamanetworkopen.2023.43410
Multimodal Analysis of Secondary Cerebellar Alterations After Pediatric Traumatic Brain Injury
Abstract
Importance: Traumatic brain injury (TBI) is known to cause widespread neural disruption in the cerebrum. However, less is known about the association of TBI with cerebellar structure and how such changes may alter executive functioning.
Objective: To investigate alterations in subregional cerebellum volume and cerebral white matter microstructure after pediatric TBI and examine subsequent changes in executive function.
Design, setting, and participants: This retrospective cohort study combined 12 data sets (collected between 2006 and 2020) from 9 sites in the Enhancing Neuroimaging Genetics Through Meta-Analysis Consortium Pediatric TBI working group in a mega-analysis of cerebellar structure. Participants with TBI or healthy controls (some with orthopedic injury) were recruited from trauma centers, clinics, and institutional trauma registries, some of which were followed longitudinally over a period of 0.7 to 1.9 years. Healthy controls were recruited from the surrounding community. Data analysis occurred from October to December 2022.
Exposure: Accidental mild complicated-severe TBI (msTBI) for those in the TBI group. Some controls received a diagnosis of orthopedic injury.
Main outcomes and measures: Volume of 18 cerebellar lobules and vermal regions were estimated from 3-dimensional T1-weighted magnetic resonance imaging (MRI) scans. White matter organization in 28 regions of interest was assessed with diffusion tensor MRI. Executive function was measured by parent-reported scores from the Behavior Rating Inventory of Executive Functioning.
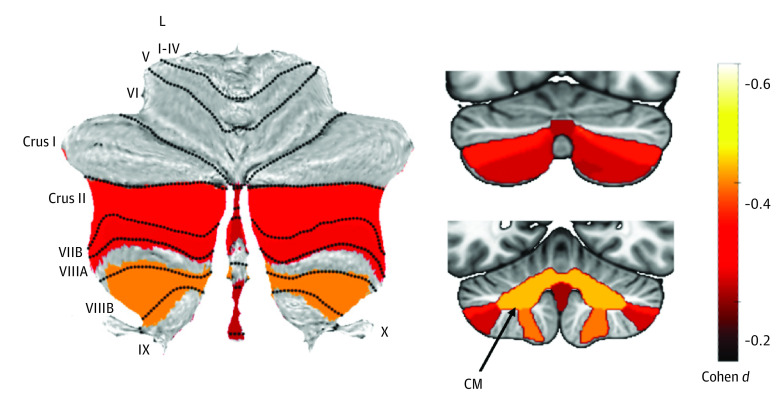
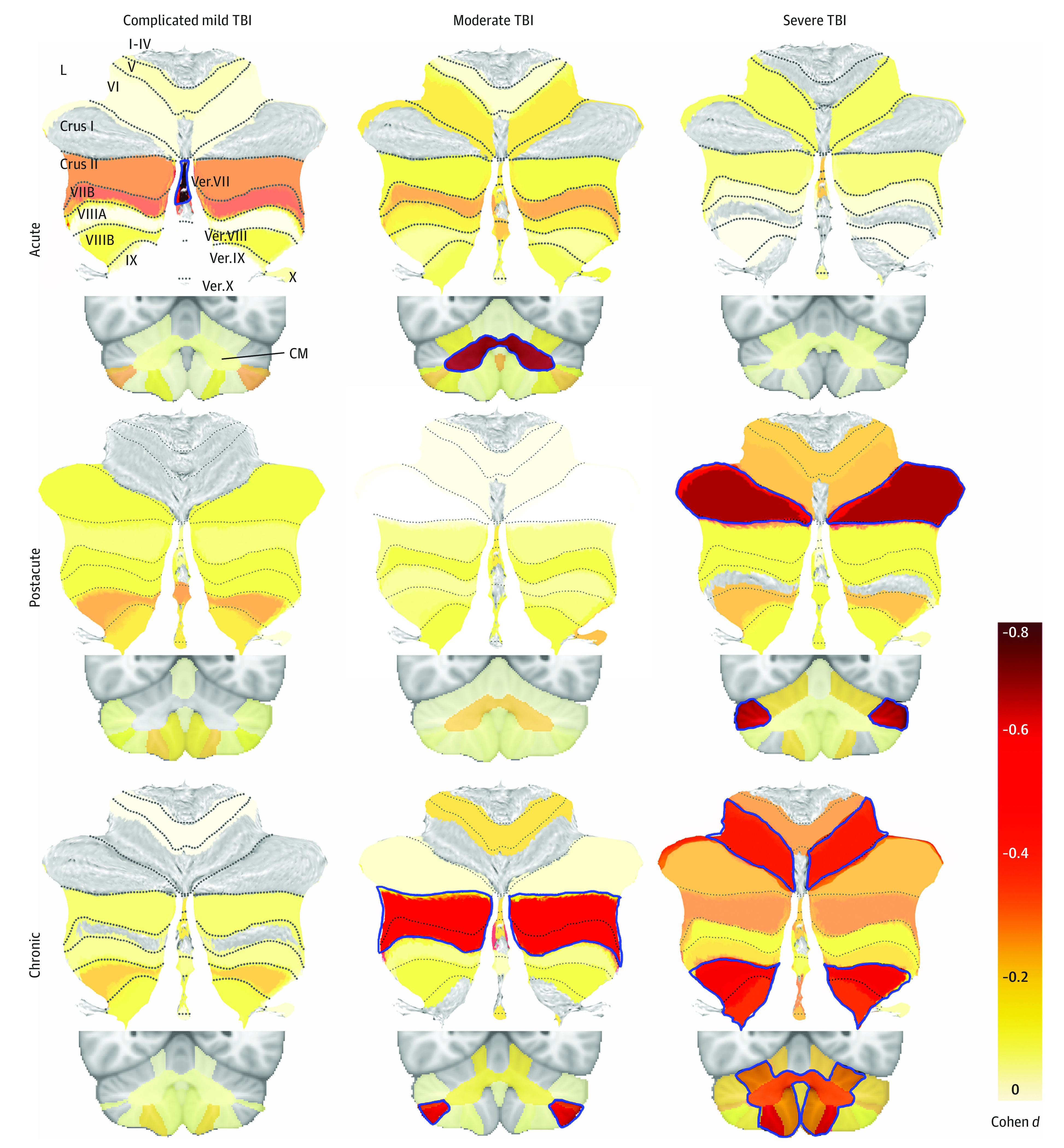
Results: A total of 598 children and adolescents (mean [SD] age, 14.05 [3.06] years; range, 5.45-19.70 years; 386 male participants [64.5%]; 212 female participants [35.5%]) were included in the study, with 314 participants in the msTBI group, and 284 participants in the non-TBI group (133 healthy individuals and 151 orthopedically injured individuals). Significantly smaller total cerebellum volume (d = -0.37; 95% CI, -0.52 to -0.22; P < .001) and subregional cerebellum volumes (eg, corpus medullare; d = -0.43; 95% CI, -0.58 to -0.28; P < .001) were observed in the msTBI group. These alterations were primarily seen in participants in the chronic phase (ie, >6 months postinjury) of injury (total cerebellar volume, d = -0.55; 95% CI, -0.75 to -0.35; P < .001). Smaller cerebellum volumes were associated with higher scores on the Behavior Rating Inventory of Executive Functioning Global Executive Composite score (β = -208.9 mm3; 95% CI, -319.0 to -98.0 mm3; P = .008) and Metacognition Index score (β = -202.5 mm3; 95% CI, -319.0 to -85.0 mm3; P = .02). In a subset of 185 participants with longitudinal data, younger msTBI participants exhibited cerebellum volume reductions (β = 0.0052 mm3; 95% CI, 0.0013 to 0.0090 mm3; P = .01), and older participants slower growth rates. Poorer white matter organization in the first months postinjury was associated with decreases in cerebellum volume over time (β=0.52 mm3; 95% CI, 0.19 to 0.84 mm3; P = .005).
Conclusions and relevance: In this cohort study of pediatric msTBI, our results demonstrated robust cerebellar volume alterations associated with pediatric TBI, localized to the posterior lobe. Furthermore, longitudinal cerebellum changes were associated with baseline diffusion tensor MRI metrics, suggesting secondary cerebellar atrophy. These results provide further understanding of secondary injury mechanisms and may point to new opportunities for intervention.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
- R61 NS120249/NS/NINDS NIH HHS/United States
- R01 HD088438/HD/NICHD NIH HHS/United States
- R01 NS122184/NS/NINDS NIH HHS/United States
- K12 HD001097/HD/NICHD NIH HHS/United States
- P50 HD103538/HD/NICHD NIH HHS/United States
- U54 EB020403/EB/NIBIB NIH HHS/United States
- R56 AG058854/AG/NIA NIH HHS/United States
- S10 OD021648/OD/NIH HHS/United States
- K01 HD083459/HD/NICHD NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- R01 NS100973/NS/NINDS NIH HHS/United States
- R01 NS110757/NS/NINDS NIH HHS/United States
- R01 MH111671/MH/NIMH NIH HHS/United States
- R01 MH116147/MH/NIMH NIH HHS/United States
- R01 HD061504/HD/NICHD NIH HHS/United States
- P41 EB015922/EB/NIBIB NIH HHS/United States
- U54 NS121688/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
