

Pembrolizumab Plus Chemotherapy Followed by Pembrolizumab in Patients With Early Triple-Negative Breast Cancer: A Secondary Analysis of a Randomized Clinical Trial
- PMID: 37966841
- PMCID: PMC10652156
- DOI: 10.1001/jamanetworkopen.2023.42107
Pembrolizumab Plus Chemotherapy Followed by Pembrolizumab in Patients With Early Triple-Negative Breast Cancer: A Secondary Analysis of a Randomized Clinical Trial
Abstract
Importance: In the phase 3 KEYNOTE-522 study, addition of pembrolizumab to neoadjuvant chemotherapy followed by adjuvant pembrolizumab significantly increased pathologic complete response (pCR) and event-free survival (EFS) vs neoadjuvant chemotherapy in patients with early triple-negative breast cancer.
Objective: To evaluate efficacy and safety outcomes for patients enrolled in East/Southeast Asia (Asia) in KEYNOTE-522.
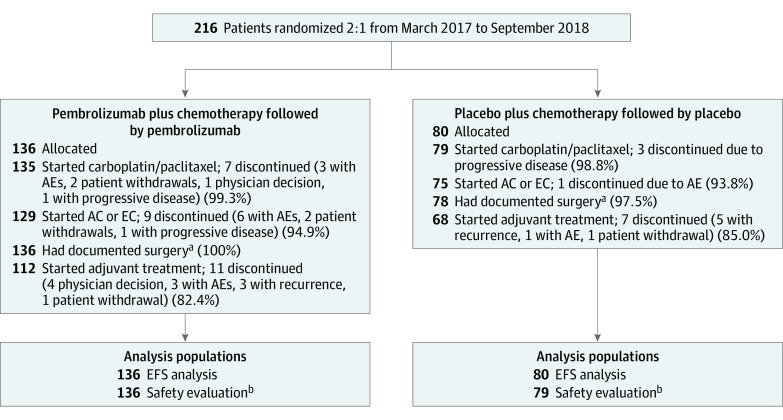
Design, setting, and participants: KEYNOTE-522, a multicenter, double-blind, randomized clinical trial, enrolled 1174 patients between March 7, 2017, and September 13, 2018. For interim EFS and overall survival (OS) analyses (data cutoff, March 23, 2021), median follow-up was 39.8 months (range, 30.4-46.9 months) for pembrolizumab plus chemotherapy and 40.8 months (range, 30.1-46.9 months) for placebo plus chemotherapy. Data cutoff for pCR analysis was September 24, 2018. This secondary analysis included adults enrolled in Asia with newly diagnosed, previously untreated, nonmetastatic triple-negative breast cancer (tumor stage T1c and nodal stage N1-2 or tumor stage T2-4 and nodal stage N0-2) and Eastern Cooperative Oncology Group performance status of 0 to 1, regardless of programmed cell death ligand 1 (PD-L1) status.
Intervention: Patients were randomized 2:1 to 4 cycles of pembrolizumab (200 mg every 3 weeks) or placebo plus carboplatin and paclitaxel and another 4 cycles of pembrolizumab or placebo plus doxorubicin or epirubicin and cyclophosphamide before surgery. After definitive surgery, patients received pembrolizumab or placebo every 3 weeks for 9 cycles or until recurrence or unacceptable toxic effects.
Main outcomes and measures: The main outcome was pCR (no evidence of primary tumor after neoadjuvant therapy or carcinoma in situ after neoadjuvant therapy and no regional lymph node involvement after neoadjuvant therapy) at the time of definitive surgery and EFS.
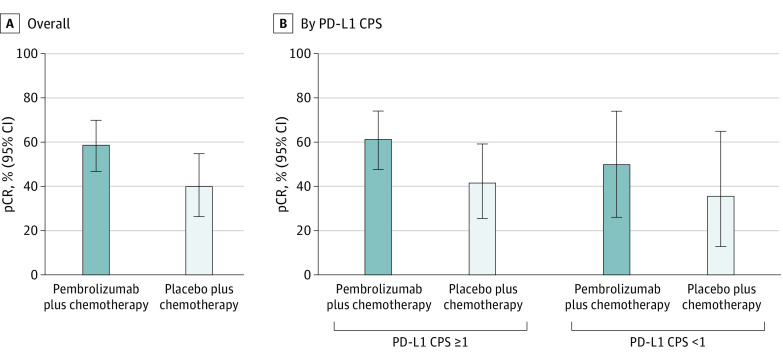
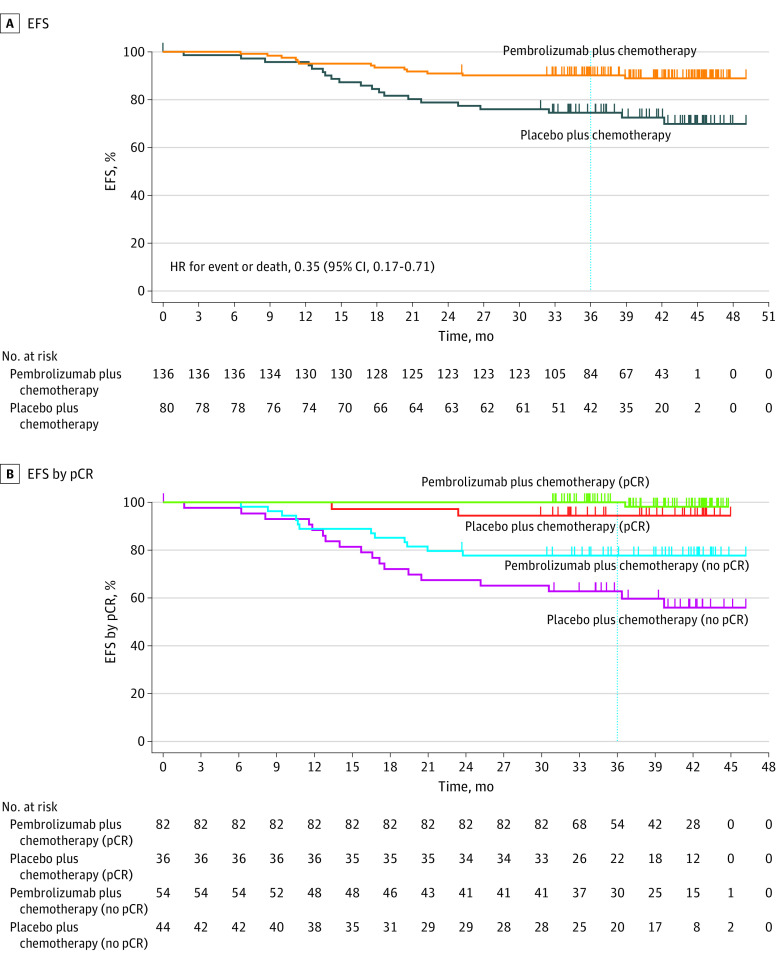
Results: A total of 216 of 1174 randomized patients (all female; median [range] age, 46.0 [24.0-71.0] years) were from Korea, Japan, Taiwan, and Singapore (136 in the pembrolizumab plus chemotherapy group and 80 in the placebo plus chemotherapy group). Of these patients, 104 (76.5%) in the pembrolizumab plus chemotherapy group and 60 (75.0%) in the placebo plus chemotherapy group had a tumor PD-L1 combined positive score of 1 or greater. Pathologic complete response was 58.7% (95% CI, 46.7%-69.9%) with pembrolizumab plus chemotherapy and 40.0% (95% CI, 26.4%-54.8%) with placebo plus chemotherapy; benefit was observed regardless of PD-L1 status. Thirteen patients (9.6%) in the pembrolizumab plus chemotherapy group and 20 patients (25.0%) in the placebo plus chemotherapy group had EFS events (hazard ratio, 0.35; 95% CI, 0.17-0.71). The 36-month EFS rate was 91.2% (95% CI, 85.0%-94.9%) with pembrolizumab plus chemotherapy and 77.2% (95% CI, 66.3%-85.0%) with placebo plus chemotherapy. Grade 3 to 4 treatment-related adverse events occurred in 109 patients (80.1%) receiving pembrolizumab plus chemotherapy and 64 patients (81.0%) receiving placebo plus chemotherapy.
Conclusions and relevance: In this subgroup analysis of patients enrolled in Asia in KEYNOTE-522, neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab led to clinically meaningful improvements in pCR and EFS vs neoadjuvant chemotherapy alone. These findings support the use of neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab as a standard-of-care therapy for patients in Asian countries with early triple-negative breast cancer.
Trial registration: ClinicalTrials.gov Identifier: NCT03036488.
Conflict of interest statement
Figures
References
-
- Garrido-Castro AC, Lin NU, Polyak K. Insights into molecular classifications of triple-negative breast cancer: improving patient selection for treatment. Cancer Discov. 2019;9(2):176-198. doi:10.1158/2159-8290.CD-18-1177 - DOI - PMC - PubMed
-
- Park YH, Senkus-Konefka E, Im SA, et al. . Pan-Asian adapted ESMO Clinical Practice Guidelines for the management of patients with early breast cancer: a KSMO-ESMO initiative endorsed by CSCO, ISMPO, JSMO, MOS, SSO and TOS. Ann Oncol. 2020;31(4):451-469. doi:10.1016/j.annonc.2020.01.008 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
