

Nodal Metastasis in Surgically Treated Oral Cavity Squamous Cell Carcinoma
- PMID: 37967536
- PMCID: PMC10652645
- DOI: 10.1159/000534491
Nodal Metastasis in Surgically Treated Oral Cavity Squamous Cell Carcinoma
Abstract
Introduction: Management of the neck in oral cavity squamous cell carcinoma (OCSCC) is essential to oncologic control and survival. The rates of lymph node metastasis (LNM) vary based on oral cavity tumor site and stage and influence treatment decisions. The aim of this paper was to describe clinical LNM for different tumor subsites and stages of surgically managed OCSCC.
Methods: We conducted a retrospective analysis of 25,846 surgically managed OCSCC patients from the National Cancer Database (NCDB) stratified by tumor subsite and clinical T-stage. For cN + patients, rates of pathologic LNM and absence of pathologic LNM were determined. For cN0 patients, outcomes included the rates of elective neck dissection (END) and occult LNM and predictors of occult LNM determined by a multivariable logistic regression model.
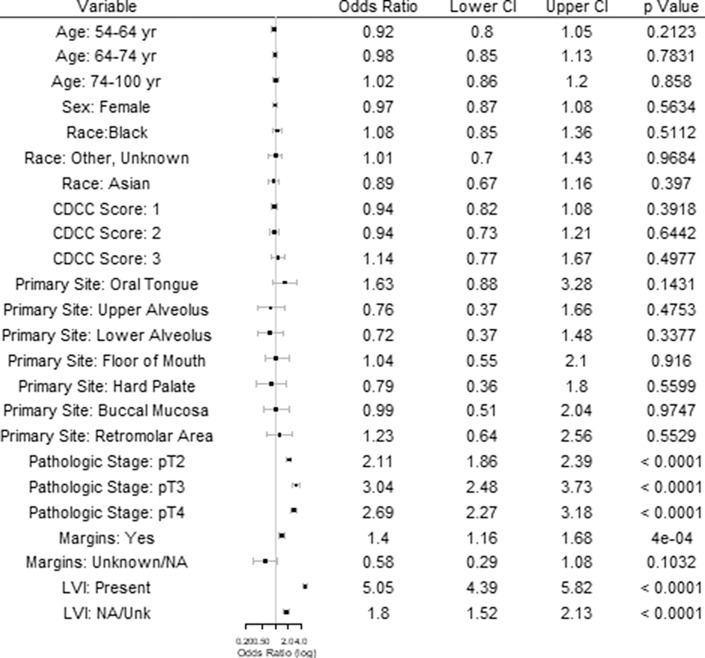
Results: A total of 25,846 patients (59.1% male, mean age 61.9 years) met inclusion criteria with primary tumor sites including oral tongue (50.8%), floor of mouth (21.2%), lower alveolus (7.6%), buccal mucosa (6.7%), retromolar area (4.9%), upper alveolus (3.6%), hard palate (2.7%), and mucosal lip (2.5%). Among all sites, clinical N+ rates increased with T-stage (8.9% T1, 28.0% T2, 51.6% T3, 52.5% T4); these trends were preserved across subsites. Among patients with cN + disease, the overall rate of concordant positive pathologic LNM was 80.1% and the rate of discordant negative pathologic LNM was 19.6%, which varied based on tumor site and stage. In the overall cohort of cN0 patients, 59.9% received END, and the percentage of patients receiving END increased with higher tumor stage. Occult LNM among those cN0 was found in 25.1% of END cases, with the highest rates in retromolar (28.8%) and oral tongue (27.5%) tumors. Multivariable regression demonstrated significantly increased rates of occult LNM for higher T stage (T2 OR: 2.1 [1.9-2.4]; T3 OR: 3.0 [2.5-3.7]; T4 OR: 2.7 [2.2-3.2]), positive margins (OR: 1.4 [1.2-1.7]), and positive lymphovascular invasion (OR: 5.1 [4.4-5.8]).
Conclusions: Management of the neck in OCSCC should be tailored based on primary tumor factors and considered for early-stage tumors.
Keywords: Head and neck; Metastasis; Neck dissection; Oral cavity; Squamous cell carcinoma.
© 2023 S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Marur S, Forastiere AA. Head and neck squamous cell carcinoma: update on Epidemiology, diagnosis, and treatment. Mayo Clin Proc. 2016 Mar;91(3):386–96. - PubMed
-
- Edge S, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, et al. . American joint committee on cancer, American cancer society, AJCC cancer staging manual. 8th ed. New York, NY: American Joint Committee on Cancer, Springer; 2017.
-
- National Comprehensive Cancer Network . Head and neck cancers (version 2.2019). https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf [accessed 16 August 2019].
-
- Yao M, Epstein JB, Modi BJ, Pytynia KB, Mundt AJ, Feldman LE. Current surgical treatment of squamous cell carcinoma of the head and neck. Oral Oncol. 2007 Mar;43(3):213–23. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
