

Comparison of surgical excision followed by adjuvant radiotherapy and laser combined with steroids for the treatment of keloids: A systematic review and meta-analysis
- PMID: 37967571
- PMCID: PMC10895202
- DOI: 10.1111/iwj.14449
Comparison of surgical excision followed by adjuvant radiotherapy and laser combined with steroids for the treatment of keloids: A systematic review and meta-analysis
Abstract
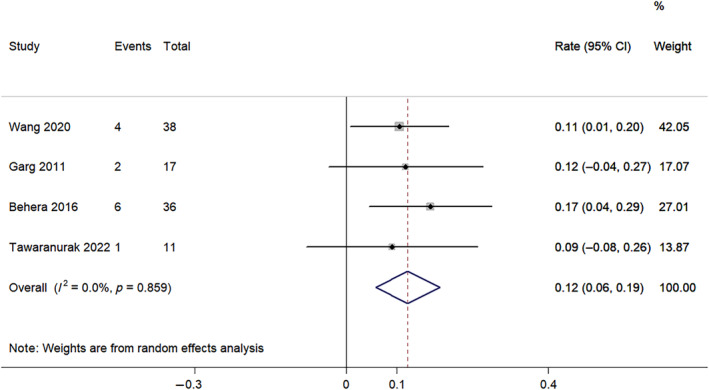
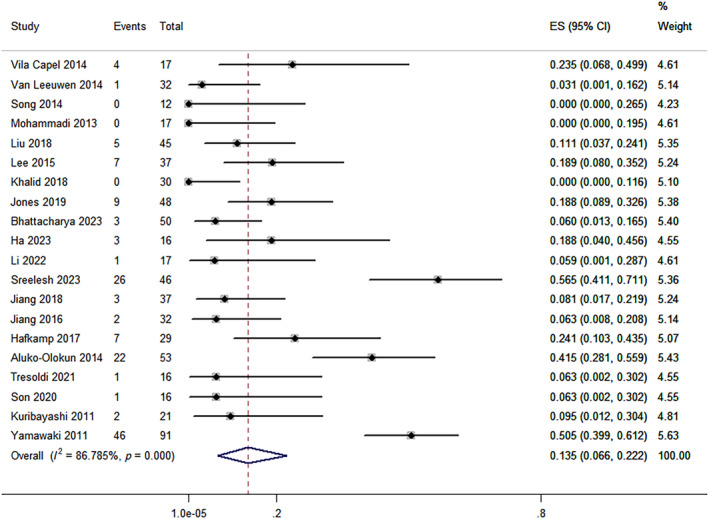
This meta-analysis aims to evaluate and compare the effect of surgical excision followed by adjuvant radiotherapy and laser combined with steroids on keloids. Relevant studies reporting the recurrence rate or incidence of adverse events (AEs) were retrieved from the PubMed, Web of Science, Embase and Cochrane Library databases through August 2023. The quality of noncomparative single-arm clinical trials was evaluated using the methodological index for nonrandomised studies (MINORS) Methodological items. This meta-analysis was conducted utilizing Stata 12.0 statistical software. 26 studies involving 989 patients were included in the analysis. The recurrence rate in the laser combined with steroids therapy group (12.2%, 95% confidence interval [CI]: 5.9%-18.5%) was lower than that of the surgical excision combined with radiotherapy group (13.5%, 95% CI: 6.6%-22.2%). For the incidence of AEs, relatively low incidence of atrophy (0.0%, 95% CI: 0.0%-1.2%), telangiectasia (3.2%, 95% CI: 0.4%-7.6%), erythema (2.3%, 95% CI: 0.0%-10.6%), infection (0.2%, 95% CI: 0.0%-1.6%) and high hyperpigmentation rate (8.3%, 95% CI: 4.2%-13.4%) were obtained in the surgical excision combined with radiotherapy group. Compared with surgical resection followed by radiotherapy, the combination of laser and steroids for keloids showed a lower hyperpigmentation rate (6.5%), as well as a higher incidence of atrophy (22.7%), telangiectasia (6.4%), erythema (3.3%) and infection (3.3%). Only a hypopigmentation rate of 2.9% was obtained in patients treated with surgical excision plus radiotherapy. Current evidence revealed that surgical excision followed by adjuvant radiotherapy and laser combined with steroids therapy were effective and safe treatments for keloids, with relatively low recurrence rate and complication rate. Comparative studies are needed to further compare the effects of these two combination therapies on keloids.
Keywords: keloid; laser; radiotherapy; steroid; surgical excision.
© 2023 The Authors. International Wound Journal published by Medicalhelplines.com Inc and John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- Flickinger JC. A radiobiological analysis of multicenter data for postoperative keloid radiotherapy. Int J Radiat Oncol Biol Phys. 2011;79(4):1164‐1170. - PubMed
-
- Li W, Wang Y, Wang X, Liu Z. A keloid edge precut, preradiotherapy method in large keloid skin graft treatment. Dermatol Surg. 2014;40(1):52‐57. - PubMed
-
- Wang J, Wu J, Xu M, et al. Combination therapy of refractory keloid with ultrapulse fractional carbon dioxide (CO2) laser and topical triamcinolone in Asians‐long‐term prevention of keloid recurrence. Dermatol Ther. 2020;33(6):e14359. - PubMed
-
- Young VL, Hutchison J. Insights into patient and clinician concerns about scar appearance: semiquantitative structured surveys. Plast Reconstr Surg. 2009;124(1):256‐265. - PubMed
-
- Tziotzios C, Profyris C, Sterling J. Cutaneous scarring: pathophysiology, molecular mechanisms, and scar reduction therapeutics part II. Strategies to reduce scar formation after dermatologic procedures. J Am Acad Dermatol. 2012;66(1):13‐24; quiz 25–16. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
