

Sleep-Related Hypoxia, Right Ventricular Dysfunction, and Survival in Patients With Group 1 Pulmonary Arterial Hypertension
- PMID: 37968017
- PMCID: PMC11060475
- DOI: 10.1016/j.jacc.2023.09.806
Sleep-Related Hypoxia, Right Ventricular Dysfunction, and Survival in Patients With Group 1 Pulmonary Arterial Hypertension
Abstract
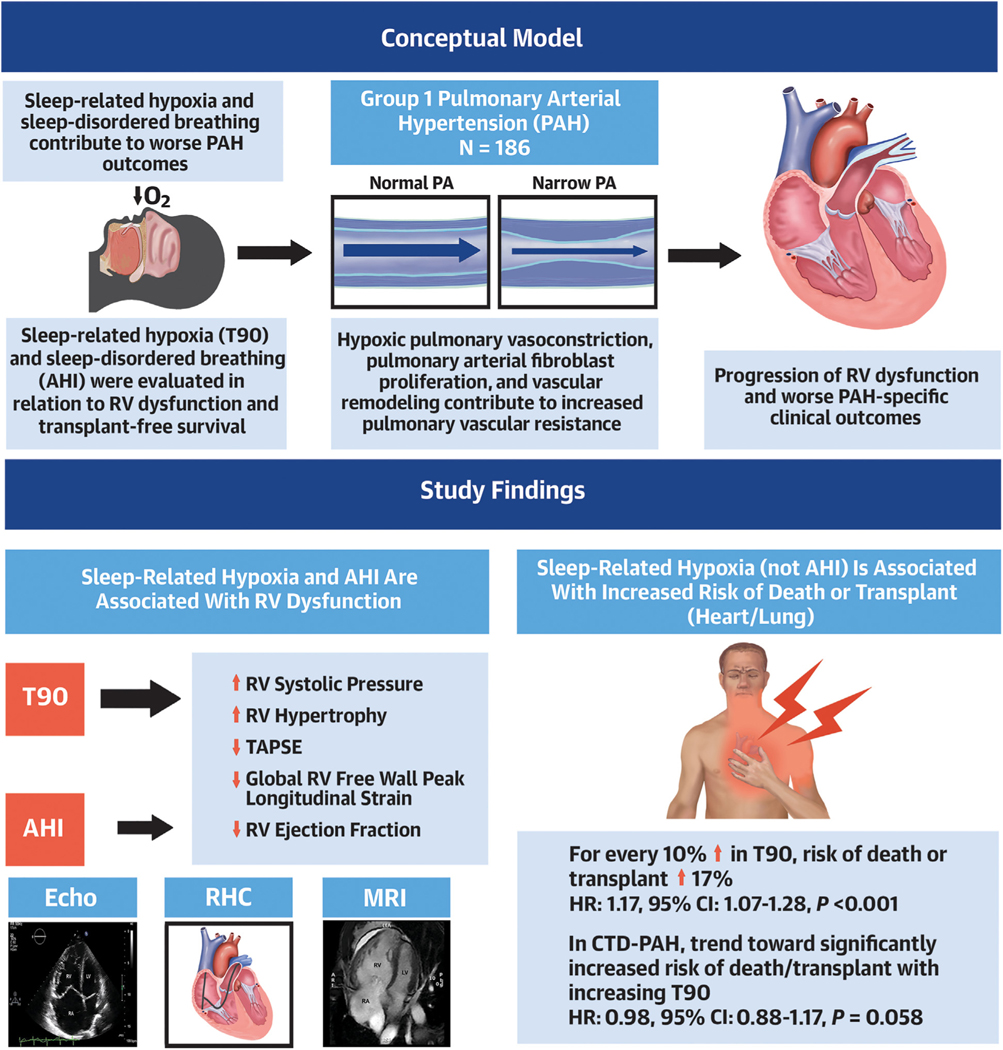
Background: Group 1 pulmonary arterial hypertension (PAH) is a progressive fatal condition characterized by right ventricular (RV) failure with worse outcomes in connective tissue disease (CTD). Obstructive sleep apnea and sleep-related hypoxia may contribute to RV dysfunction, though the relationship remains unclear.
Objectives: The aim of this study was to prospectively evaluate the association of the apnea-hypopnea index (AHI) and sleep-related hypoxia with RV function and survival.
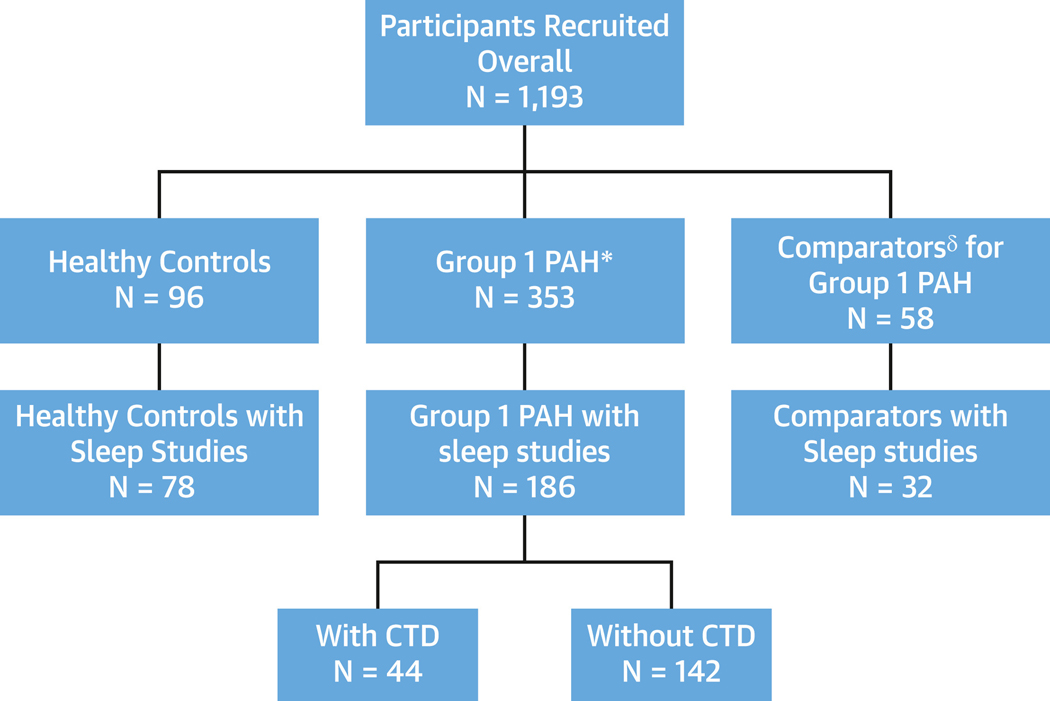
Methods: Pulmonary Vascular Disease Phenomics (National Heart, Lung, and Blood Institute) cohort participants (patients with group 1 PAH, comparators, and healthy control participants) with sleep studies were included. Multimodal RV functional measures were examined in association with AHI and percentage of recording time with oxygen saturation <90% (T90) per 10-unit increment. Linear models, adjusted for demographics, oxygen, diffusing capacity of the lungs for carbon monoxide, pulmonary hypertension medications, assessed AHI and T90, and RV measures. Log-rank test/Cox proportional hazards models adjusted for demographics, oxygen, and positive airway pressure were constructed for transplantation-free survival analyses.
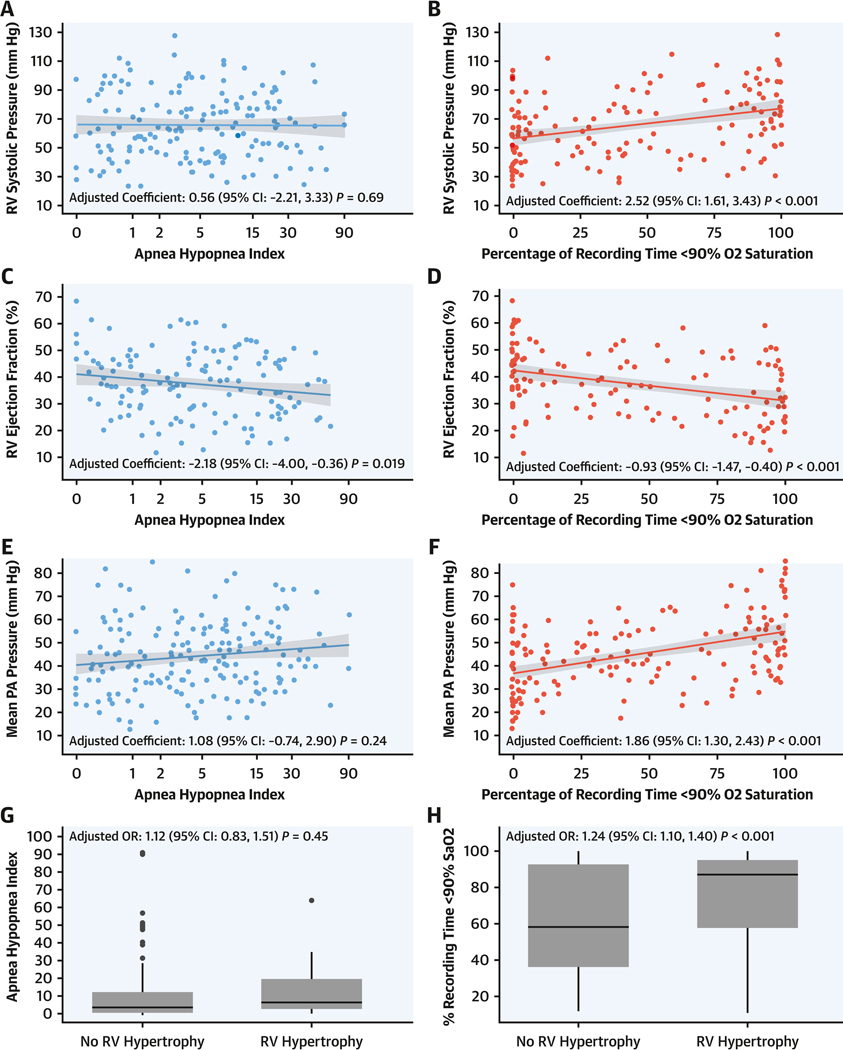
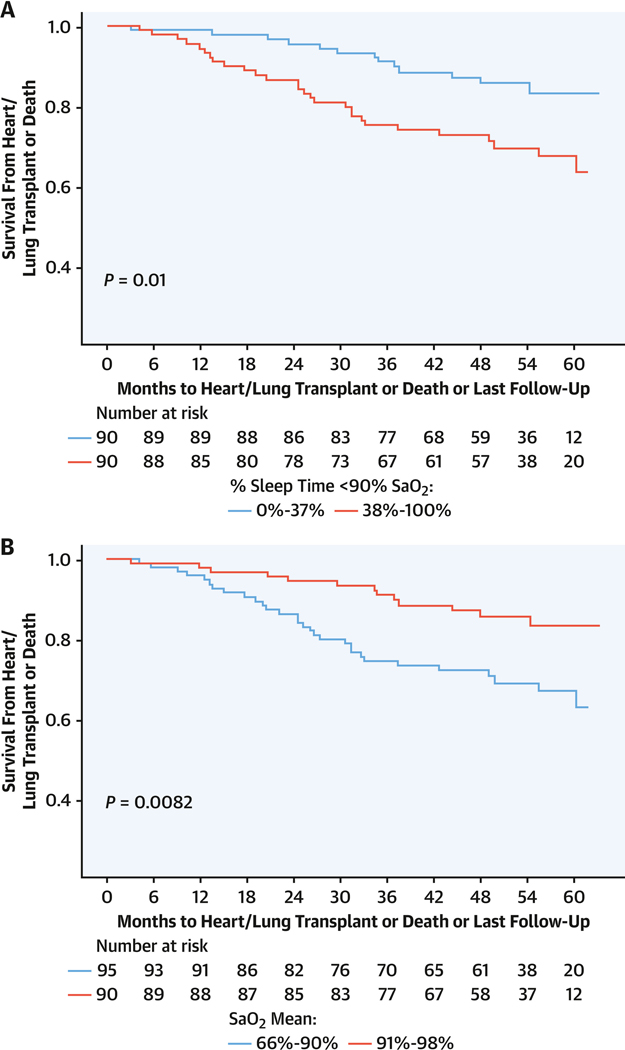
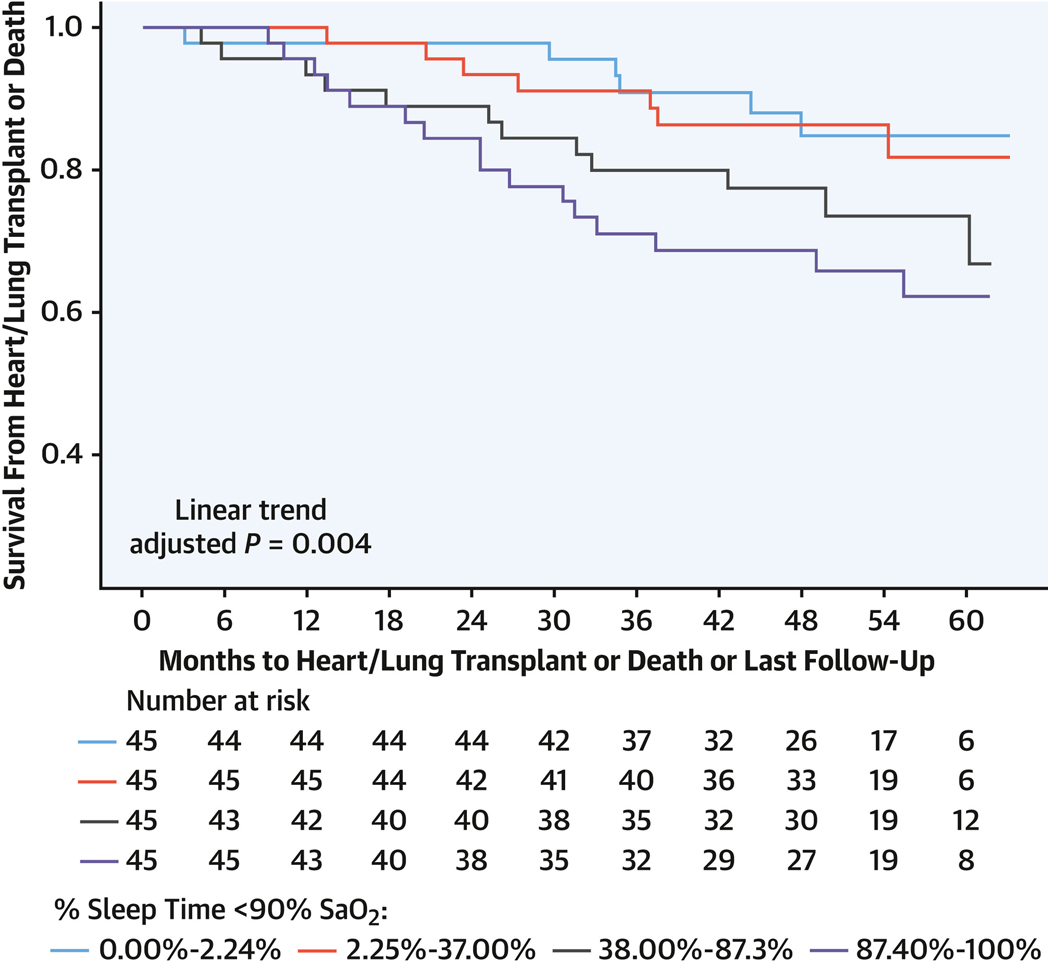
Results: Analysis included 186 participants with group 1 PAH with a mean age of 52.6 ± 14.1 years; 71.5% were women, 80.8% were Caucasian, and there were 43 events (transplantation or death). AHI and T90 were associated with decreased RV ejection fraction (on magnetic resonance imaging), by 2.18% (-2.18; 95% CI: -4.00 to -0.36; P = 0.019) and 0.93% (-0.93; 95% CI: -1.47 to -0.40; P < 0.001), respectively. T90 was associated with increased RV systolic pressure (on echocardiography), by 2.52 mm Hg (2.52; 95% CI: 1.61 to 3.43; P < 0.001); increased mean pulmonary artery pressure (on right heart catheterization), by 0.27 mm Hg (0.27; 95% CI: 0.05 to 0.49; P = 0.019); and RV hypertrophy (on electrocardiography), 1.24 mm (1.24; 95% CI: 1.10 to 1.40; P < 0.001). T90, but not AHI, was associated with a 17% increased 5-year risk for transplantation or death (HR: 1.17; 95% CI: 1.07 to 1.28). In non-CTD-associated PAH, T90 was associated with a 21% increased risk for transplantation or death (HR: 1.21; 95% CI: 1.08 to 1.34). In CTD-associated PAH, T90 was associated with RV dysfunction, but not death or transplantation.
Conclusions: Sleep-related hypoxia was more strongly associated than AHI with measures of RV dysfunction, death, or transplantation overall and in group 1 non-CTD-associated PAH but only with RV dysfunction in CTD-associated PAH. (Pulmonary Vascular Disease Phenomics Program [PVDOMICS]; NCT02980887).
Keywords: connective tissue disease–associated pulmonary arterial hypertension; obstructive sleep apnea; pulmonary arterial hypertension; pulmonary hypertension; right ventricular dysfunction; sleep-related hypoxia.
Copyright © 2023 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was supported by grants U01 HL125218 (principal investigator, Dr Rosenzweig), U01 HL125205 (principal investigator, Dr Frantz), U01 HL125212 (principal investigator, Dr Hemnes), U01 HL125208 (principal investigator, Dr Rischard), U01 HL125175 (principal investigator, Dr Hassoun), U01 HL125215 (principal investigator, Dr Leopold), and U01 HL125177 (principal investigator, Dr Beck) and the Pulmonary Hypertension Association. Dr Hill is a scientific advisory board member for Aerovate and Insmed; is a consultant for Bellerophon; and is a data and safety monitoring board member for Merck. Dr Finet has served as a clinical practice advisor for Wolters Kluwer Health-Lexicomp (forfeited compensation); and is an Item-Writing Task Force member for the American Board of Internal Medicine. Dr Kwon has received funding from the National Heart, Lung, and Blood Institute (grant 1R01HL170090-01); and has a research agreement with Circle Cardiovascular Imaging. Dr Beck has received support from the Pulmonary Hypertension Association. Dr Frantz has consulting, steering committee, and advisory board relationships with Altavant Sciences, Bayer, Gossamer Bio, Janssen, Shouti, the France Foundation, IQVIA, Tenax, UpToDate, and United Therapeutics. Dr Hassoun serves on a scientific steering committee for Merck Sharpe & Dohme; and is a scientific adviser for ARIA-CV (unrelated to the present work). Dr Hemnes serves as a consultant for Bayer, United Therapeutics, Janssen, GossamerBio, and Tenax Therapeutics; holds stock in Tenax Therapeutics; and has received grants from the National Institutes of Health, the Cardiovascular Medical Research and Education Fund, and Imara. Dr Horn has conducted research studies with Acceleron/Merck, Cereno, and Insmed. Dr Leopold is a consultant for Abbott Vascular; is a speaker for United Therapeutics; has received research funding from Astellas to her institution; and has received support from the American Heart Association (grant AIM 19AIML34980000; National Heart, Lung, and Blood Institute grant U01 HL125215). Dr Rischard has consulting relationships with Acceleron and United Therapeutics; is a steering committee member for Acceleron; and receives research support from Ismed, United Therapeutics, Bayer, Acceleron, Janssen, and Aadi Bioscience. Dr Mehra has received an honorarium from the American Academy of Sleep Medicine; has received funds for service on the American Board of Internal Medicine and as associate editor of the American Journal of Respiratory and Critical Care Medicine; has received National Institutes of Health funding; has received investigator-initiated research funds to her institution from Resmed, Inspire, and Sommetrics; and has received royalties from UpToDate. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Sleep, Hypoxia, and Survival in Group 1 Pulmonary Arterial Hypertension: What to Do?J Am Coll Cardiol. 2023 Nov 21;82(21):2006-2008. doi: 10.1016/j.jacc.2023.10.005. J Am Coll Cardiol. 2023. PMID: 37968018 No abstract available.
References
-
- Humbert M, Sitbon O, Yaïci A, et al. Survival in incident and prevalent cohorts of patients with pulmonary arterial hypertension. Eur Respir J. 2010;36(3):549–555. - PubMed
-
- Rådegran G, Kjellström B, Ekmehag B, et al. Characteristics and survival of adult Swedish PAH and CTEPH patients 2000–2014. Scand Cardiovasc J. 2016;50(4):243–250. - PubMed
-
- Benza RL, Miller DP, Barst RJ, Badesch DB, Frost AE, McGoon MD. An evaluation of long-term survival from time of diagnosis in pulmonary arterial hypertension from the REVEAL registry. Chest. 2012;142(2):448–456. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
