

CD201+ fascia progenitors choreograph injury repair
- PMID: 37968392
- PMCID: PMC10665192
- DOI: 10.1038/s41586-023-06725-x
CD201+ fascia progenitors choreograph injury repair
Erratum in
-
Author Correction: CD201+ fascia progenitors choreograph injury repair.Nature. 2024 Jan;625(7993):E4. doi: 10.1038/s41586-023-06928-2. Nature. 2024. PMID: 38057669 Free PMC article. No abstract available.
Abstract
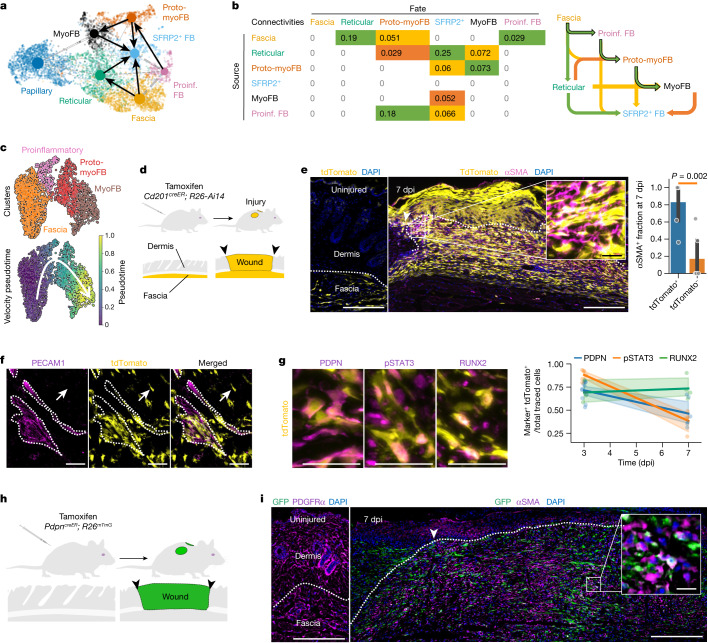
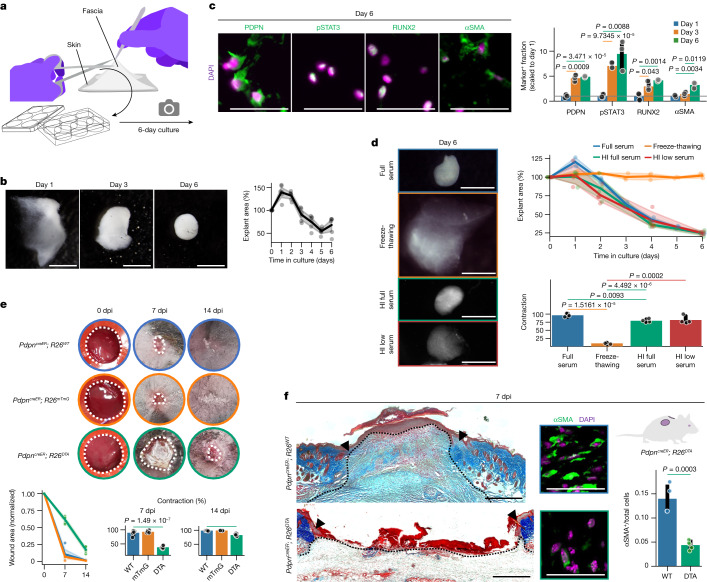
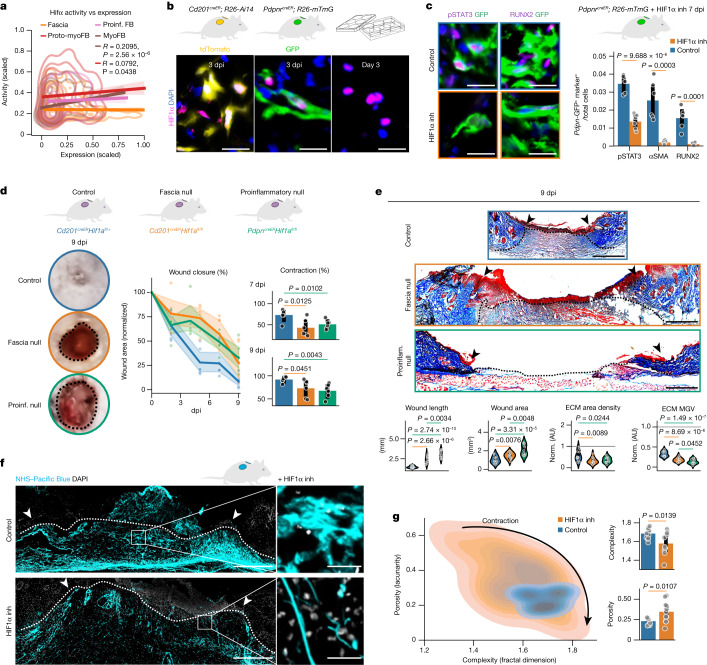
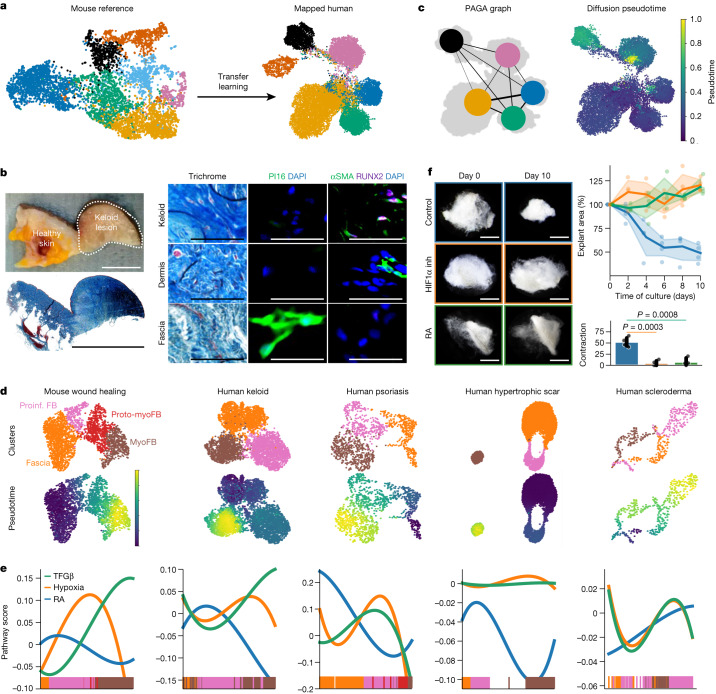
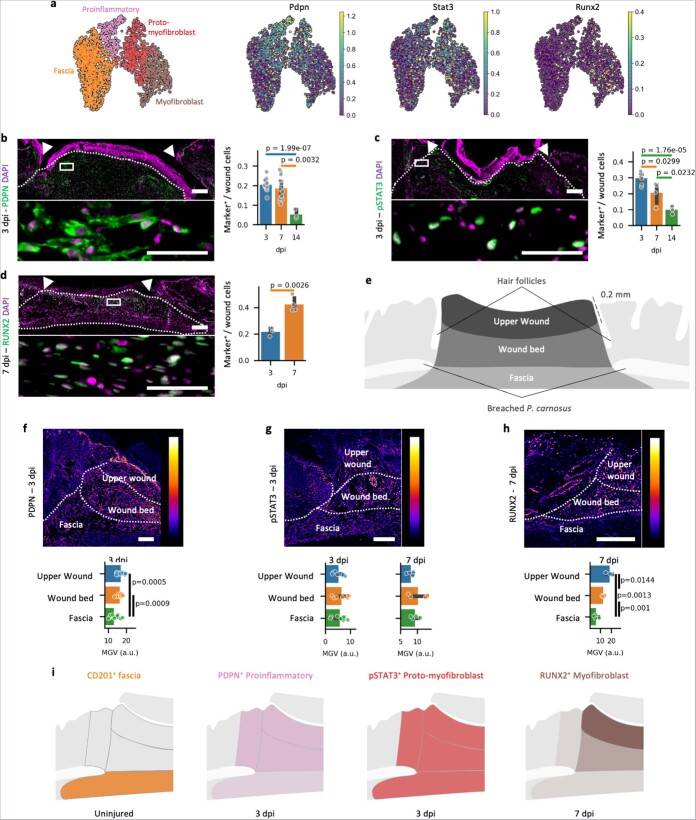
Optimal tissue recovery and organismal survival are achieved by spatiotemporal tuning of tissue inflammation, contraction and scar formation1. Here we identify a multipotent fibroblast progenitor marked by CD201 expression in the fascia, the deepest connective tissue layer of the skin. Using skin injury models in mice, single-cell transcriptomics and genetic lineage tracing, ablation and gene deletion models, we demonstrate that CD201+ progenitors control the pace of wound healing by generating multiple specialized cell types, from proinflammatory fibroblasts to myofibroblasts, in a spatiotemporally tuned sequence. We identified retinoic acid and hypoxia signalling as the entry checkpoints into proinflammatory and myofibroblast states. Modulating CD201+ progenitor differentiation impaired the spatiotemporal appearances of fibroblasts and chronically delayed wound healing. The discovery of proinflammatory and myofibroblast progenitors and their differentiation pathways provide a new roadmap to understand and clinically treat impaired wound healing.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures










References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
