

Predicting glaucoma progression using deep learning framework guided by generative algorithm
- PMID: 37968437
- PMCID: PMC10651936
- DOI: 10.1038/s41598-023-46253-2
Predicting glaucoma progression using deep learning framework guided by generative algorithm
Abstract
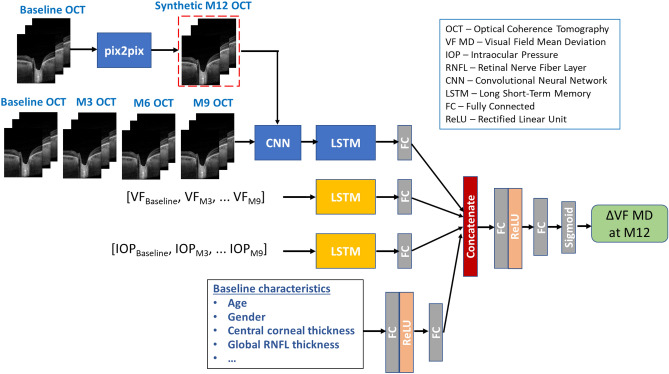
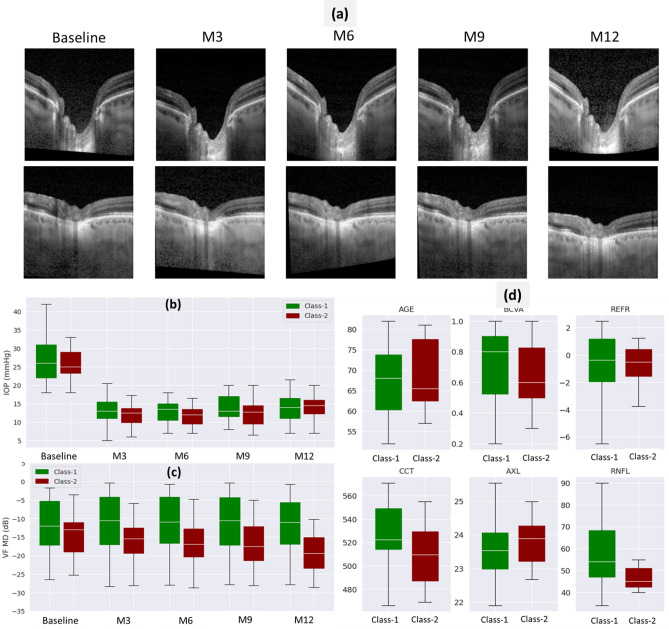
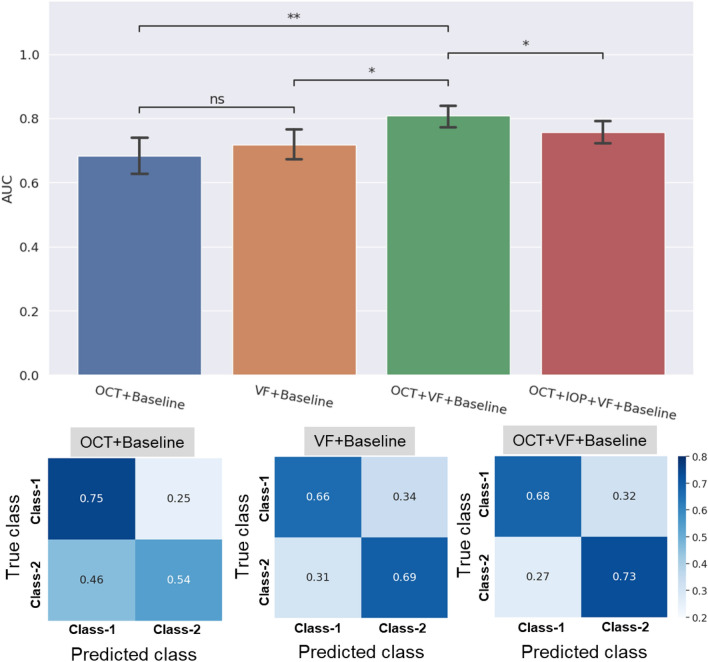
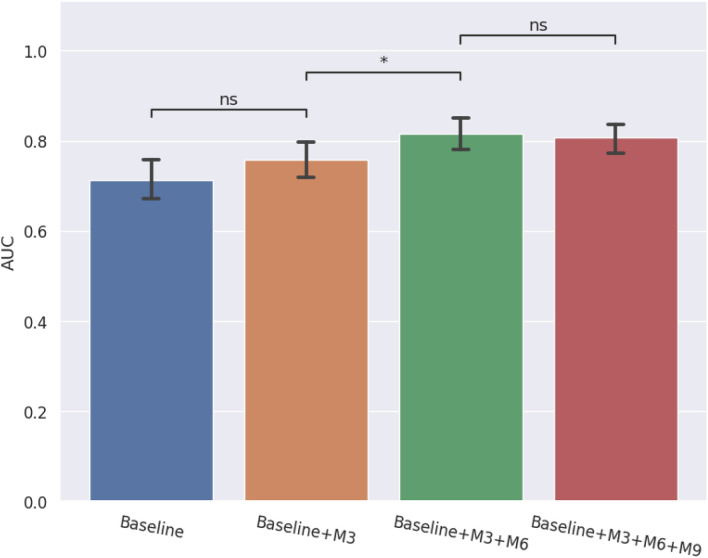
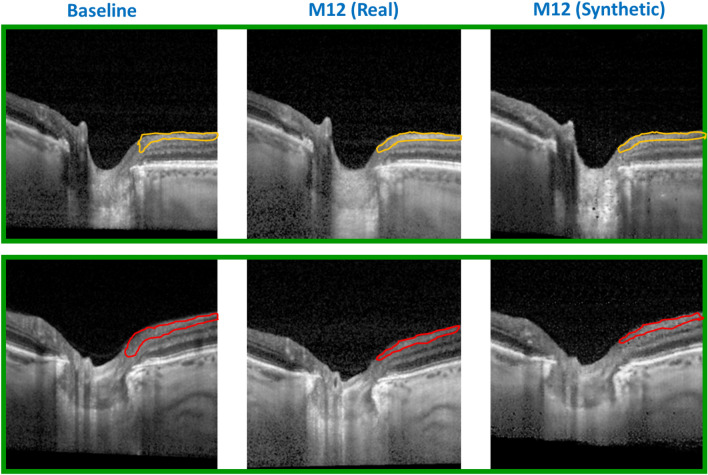
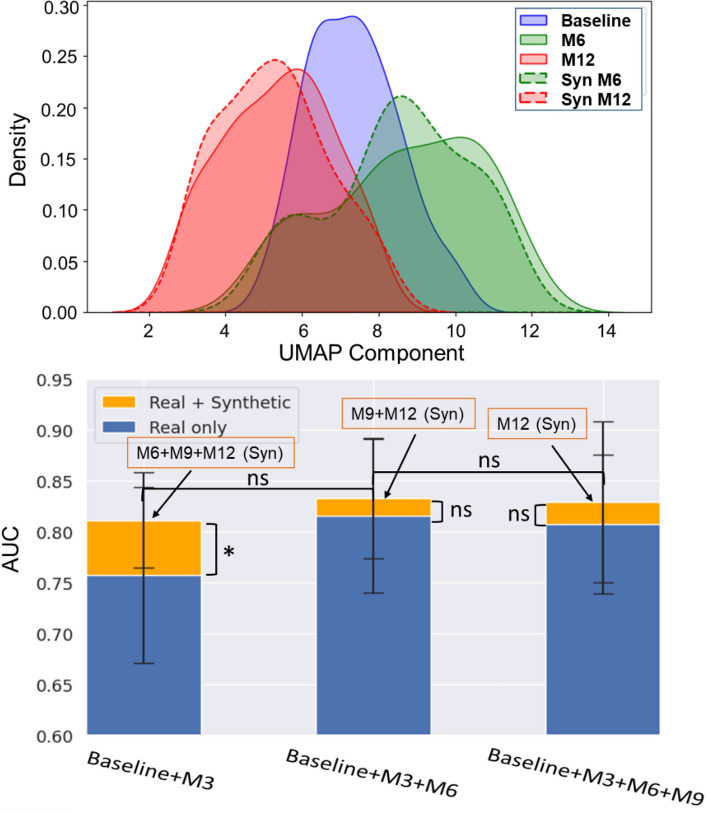
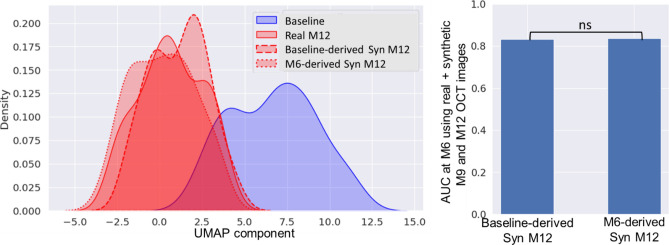
Glaucoma is a slowly progressing optic neuropathy that may eventually lead to blindness. To help patients receive customized treatment, predicting how quickly the disease will progress is important. Structural assessment using optical coherence tomography (OCT) can be used to visualize glaucomatous optic nerve and retinal damage, while functional visual field (VF) tests can be used to measure the extent of vision loss. However, VF testing is patient-dependent and highly inconsistent, making it difficult to track glaucoma progression. In this work, we developed a multimodal deep learning model comprising a convolutional neural network (CNN) and a long short-term memory (LSTM) network, for glaucoma progression prediction. We used OCT images, VF values, demographic and clinical data of 86 glaucoma patients with five visits over 12 months. The proposed method was used to predict VF changes 12 months after the first visit by combining past multimodal inputs with synthesized future images generated using generative adversarial network (GAN). The patients were classified into two classes based on their VF mean deviation (MD) decline: slow progressors (< 3 dB) and fast progressors (> 3 dB). We showed that our generative model-based novel approach can achieve the best AUC of 0.83 for predicting the progression 6 months earlier. Further, the use of synthetic future images enabled the model to accurately predict the vision loss even earlier (9 months earlier) with an AUC of 0.81, compared to using only structural (AUC = 0.68) or only functional measures (AUC = 0.72). This study provides valuable insights into the potential of using synthetic follow-up OCT images for early detection of glaucoma progression.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
