

Population-level effectiveness of alternative approaches to preventing mental disorders in adolescents and young adults
- PMID: 37968445
- PMCID: PMC10652005
- DOI: 10.1038/s41598-023-47322-2
Population-level effectiveness of alternative approaches to preventing mental disorders in adolescents and young adults
Abstract
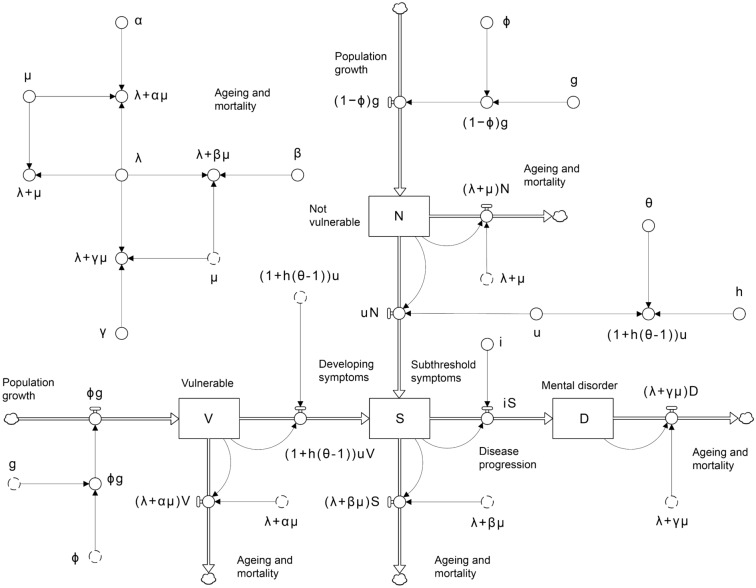
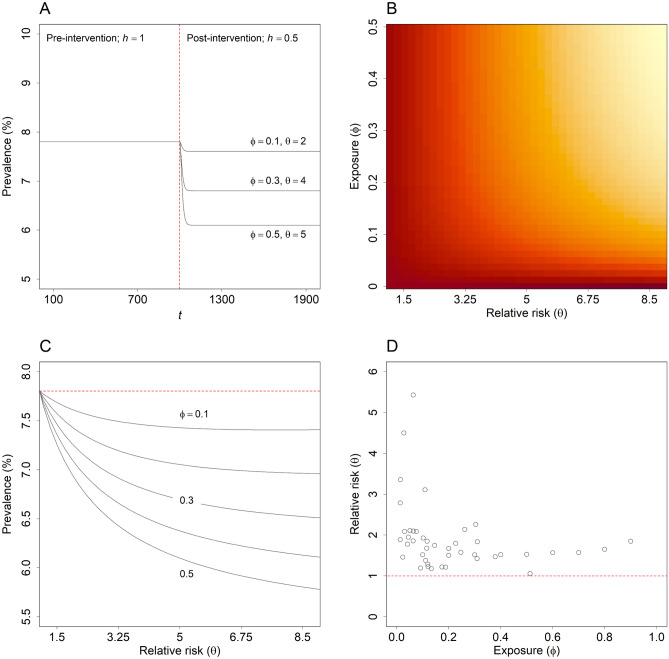
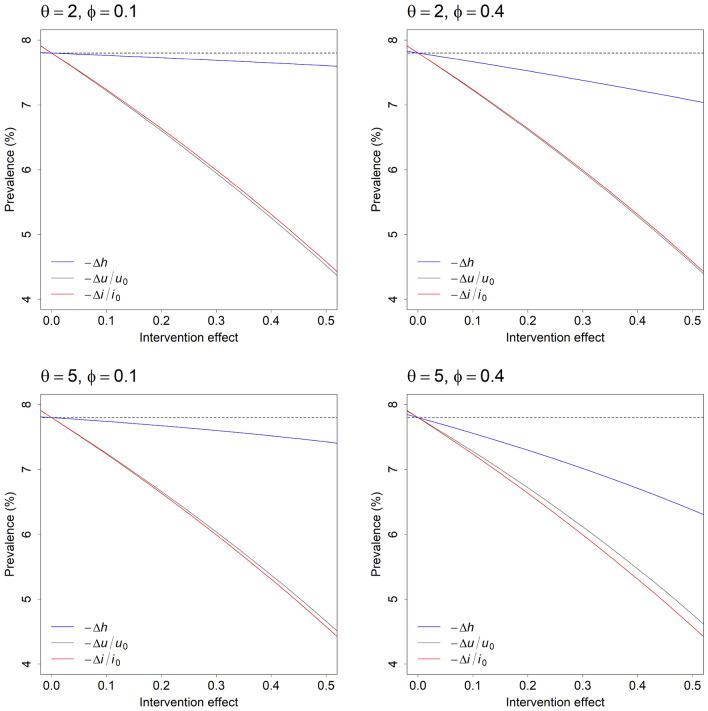
Preventive interventions that are effective in reducing the incidence of mental disorders in adolescence and early adulthood may impact substantially on lifetime economic, educational, and health outcomes; however, relatively few studies have examined the capacity of alternative approaches to preventing youth mental disorders (specifically, universal, selective, and indicated prevention) to reduce disorder incidence at a population level. Using a dynamic model of the onset of non-specific, relatively mild symptoms and progression to more severe disease, we show that: (1) indicated preventive interventions, targeting adolescents and young adults experiencing subthreshold symptoms, may often be more effective in reducing mental disorder prevalence than universal interventions delivered to the general population (contrary to the widely accepted view that a 'high risk' prevention strategy, focussing on those individuals with the greatest risk of developing a disorder, will generally be less effective than a whole-population strategy); and (2) the ability of selective preventive interventions (targeting vulnerable, asymptomatic youth) to alter the prevalence of mental disorders is severely restricted by an inverse relationship between the prevalence of significant risk factors for mental illness and the relative risk of developing symptoms.
© 2023. The Author(s).
Conflict of interest statement
Associate Professor Jo-An Occhipinti is Head of Systems Modelling, Simulation & Data Science at the Brain and Mind Centre, University of Sydney and Managing Director of Computer Simulation and Advanced Research Technologies (CSART). Professor Ian Hickie (IBH) was an inaugural Commissioner on Australia’s National Mental Health Commission (2012−18). He is the Co-Director, Health and Policy at the Brain and Mind Centre, University of Sydney. The Brain and Mind Centre operates an early-intervention youth service at Camperdown under contract to headspace. IBH has previously led community-based and pharmaceutical industry-supported (Wyeth, Eli Lily, Servier, Pfizer, AstraZeneca) projects focused on the identification and better management of anxiety and depression. He was a member of the Medical Advisory Panel for Medibank Private until October 2017, a Board Member of Psychosis Australia Trust, and a member of Veterans Mental Health Clinical Reference group. He is the Chief Scientific Advisor to, and a 3.2% equity shareholder in, InnoWell Pty Ltd. InnoWell was formed by the University of Sydney (45% equity) and PwC (Australia; 45% equity) to deliver the $30 M Australian Government-funded Project Synergy (2017−20; a three-year program for the transformation of mental health services) and to lead transformation of mental health services internationally through the use of innovative technologies. Dr Adam Skinner (AS) and Dr Yun Ju Christine Song (YJCS) declare no competing interests.
Figures
References
-
- Solmi M, Radua J, Olivola M, Croce E, Soardo L, de Pablo GS, Shin JI, Kirkbride JB, Jones P, Kim JH, Kim JY, Carvalho AF, Seeman MV, Correll CU, Fusar-Poli P. Age of onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatry. 2022;27:281–295. doi: 10.1038/s41380-021-01161-7. - DOI - PMC - PubMed
-
- Patton GC, Sawyer SM, Santelli JS, Ross DA, Afifi R, Allen NB, Arora M, Azzopardi P, Baldwin W, Bonell C, Kakuma R, Kennedy E, Mahon J, McGovern T, Mokdad AH, Patel V, Petroni S, Reavley N, Taiwo K, Waldfogel J, Wickremarathne D, Barroso C, Bhutta Z, Fatusi AO, Mattoo A, Diers J, Fang J, Ferguson J, Ssewamala F, Viner RM. Our future: a Lancet commission on adolescent health and wellbeing. Lancet. 2016;387:2423–2478. doi: 10.1016/S0140-6736(16)00579-1. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
