

Associations between types and sources of dietary carbohydrates and liver fat: a UK Biobank study
- PMID: 37968623
- PMCID: PMC10652437
- DOI: 10.1186/s12916-023-03135-8
Associations between types and sources of dietary carbohydrates and liver fat: a UK Biobank study
Abstract
Background and aims: Excess energy intake can lead to metabolic dysfunction-associated steatotic liver disease (MASLD), but the relationship between dietary carbohydrate intake and liver fat content remains unclear. This study aimed to examine the associations between types and sources of dietary carbohydrates and liver fat content.
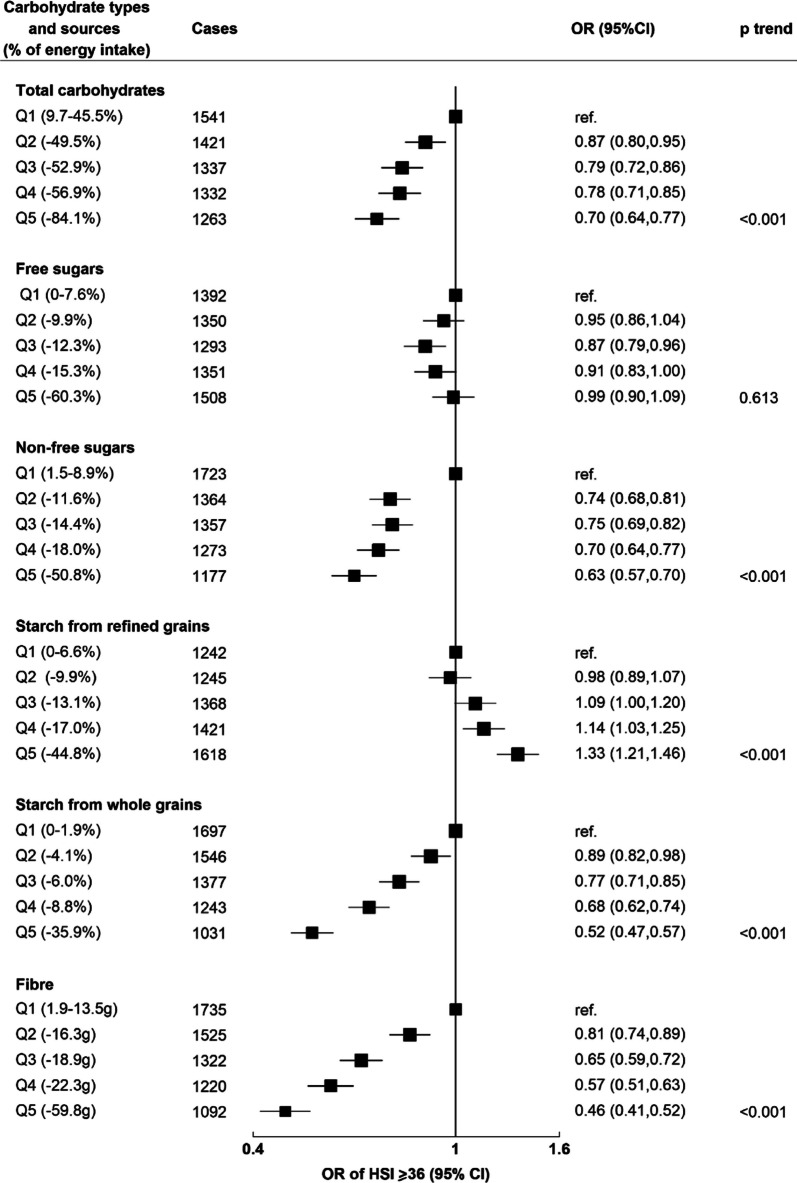
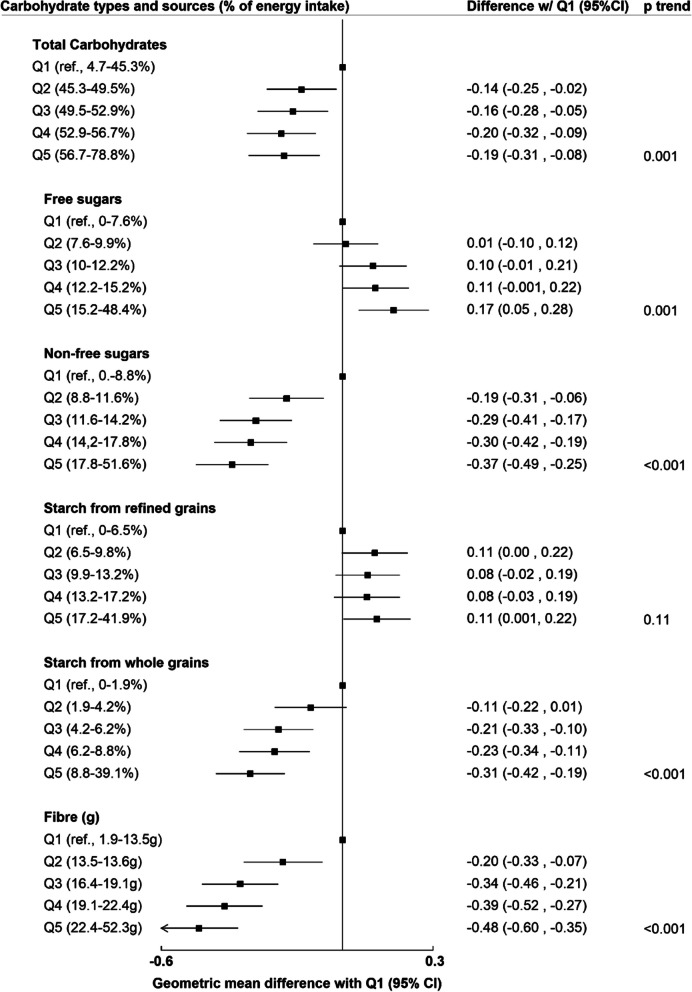
Methods: UK Biobank participants with no pre-existing diabetes, liver disease or cardiovascular disease reported dietary intake of types and sources of carbohydrates (total carbohydrates, free sugars, non-free sugars, starch from whole grains, starch from refined grains, and fibre) on at least two 24-h dietary assessments. In cross-sectional analyses, (n = 22,973), odds ratios (OR) of high liver fat content (defined as a score of ≥ 36 in the hepatic steatosis index) by quintiles of carbohydrate intakes were estimated using multivariable logistic regression models. In prospective analyses, a second sample (n = 9268) had liver proton density fat fraction (PDFF) measured by magnetic resonance imaging (2014-2020). Multivariable linear regression models estimated geometric means of PDFF (%) by quintiles of carbohydrate intakes. Models were adjusted for demographic and lifestyle confounders, including total energy intake.
Results: In the cross-sectional analyses, 6894 cases of high liver fat content were identified. Inverse associations between intakes of fibre (OR of highest vs. lowest quintile 0.46 [95% CI: 0.41-0.52]), non-free sugars (0.63 [0.57-0.70]) and starch from whole grains (0.52 [0.47-0.57]) with liver fat were observed. There were positive associations between starch from refined grains and liver fat (1.33 [1.21-1.46]), but no association with free sugars (p=0.61). In prospective analyses, inverse associations with PDFF (%) were observed for intakes of fibre (- 0.48 geometric mean difference between highest and lowest quintile of intake [- 0.60 to - 0.35]), non-free sugars (- 0.37 [- 0.49 to - 0.25]) and starch from whole grains (- 0.31 [- 0.42 to - 0.19]). Free sugars, but not starch from refined grains, were positively associated with PDFF (0.17 [0.05 to 0.28]).
Conclusion: This study suggests that different carbohydrate types and sources have varying associations with liver fat, which may be important for MASLD prevention. Non-free sugars, fibre, and starch from whole grains could be protective, while associations with free sugars and starch from refined grains are less clear.
Keywords: Carbohydrate quality; Dietary carbohydrates; Fibre intake; Hepatic steatosis; MASLD; Non-alcoholic fatty liver.
© 2023. The Author(s).
Conflict of interest statement
DAK has been the chief investigator in two publicly funded (NIHR) trials where the weight loss intervention was donated by Nestle Health Sciences to the University of Oxford outside the submitted work. The other authors declare no competing interests.
Figures
References
-
- Rinella ME, Lazarus JV, Ratziu V, Francque SM, Sanyal AJ, Kanwal F, et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
