

Approach to Wide Complex Tachycardia in Paediatric Patients
- PMID: 37969244
- PMCID: PMC10642107
- DOI: 10.1016/j.cjcpc.2022.02.003
Approach to Wide Complex Tachycardia in Paediatric Patients
Abstract
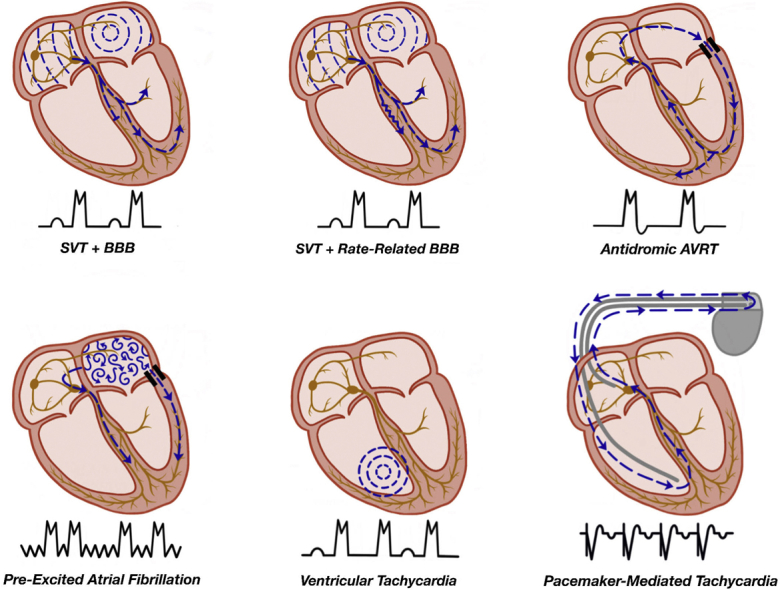
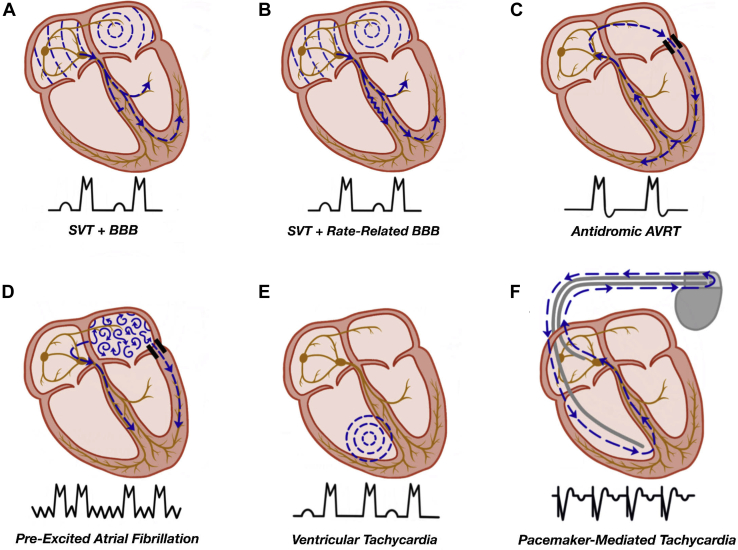
Wide complex tachycardia (WCT) is an infrequently encountered condition in paediatric patients and may be due to a variety of causes including supraventricular tachycardia with aberrant conduction, ventricular activation via an accessory pathway, ventricular pacing, or ventricular tachycardia. Immediate tachycardia termination is required in haemodynamically unstable patients. After stabilization or in those with haemodynamically tolerated WCT, a careful review of electrocardiographic tracings and diagnostic manoeuvres are essential to help elucidate the cause. Subacute and chronic management for WCT will depend on the underlying cause as well as features of the patient and the tachycardia presentation. This article will review the epidemiology, potential causes, and management of WCT in children. A detailed review of the pathophysiology, differential diagnosis, and diagnostic and treatment options is provided to enable the reader to develop a practical approach to managing this condition in young patients.
La tachycardie à complexes QRS larges est rare en pédiatrie et peut avoir diverses causes, notamment une tachycardie supraventriculaire avec trouble de la conduction, l’activation ventriculaire par une voie accessoire, une stimulation ventriculaire ou une tachycardie ventriculaire. La suppression immédiate de la tachycardie est primordiale lorsque l’état hémodynamique du patient est instable. Une fois l’état du patient stabilisé, ou en cas de tachycardie à complexes QRS larges tolérée sur le plan hémodynamique, l’examen minutieux des tracés électrocardiographiques et des manœuvres diagnostiques est crucial pour en élucider la cause. La prise en charge des cas subaigus et chroniques de tachycardie à complexes QRS larges dépend de sa cause sous-jacente ainsi que des caractéristiques du patient et du tableau clinique de la tachycardie. Cet article porte sur l’épidémiologie, les causes possibles et la prise en charge de la tachycardie à complexes QRS larges chez les enfants. Un examen approfondi de la physiopathologie, du diagnostic différentiel et des options diagnostiques et thérapeutiques est présenté pour permettre au lecteur d’élaborer une approche pratique pour la prise en charge de cette affection chez leurs jeunes patients.
© 2022 The Author(s).
Figures




References
-
- Salerno J.C., Seslar S.P. Supraventricular tachycardia. Arch Pediatr Adolesc Med. 2009;163:268–274. - PubMed
-
- Roggen A., Pavlovic M., Pfammatter J.P. Frequency of spontaneous ventricular tachycardia in a pediatric population. Am J Cardiol. 2008;101:852–854. - PubMed
-
- Ceresnak S.R., Liberman L., Avasarala K., et al. Are wide complex tachycardia algorithms applicable in children and patients with congenital heart disease? J Electrocardiol. 2010;43:694–854. - PubMed
-
- Topjian A.A., Raymond T.T., Atkins D., et al. Part 4: pediatric basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142(suppl 2):469–523. - PubMed
-
- Crosson J.E., Callans D.J., Bradley D.J., et al. PACES/HRS expert consensus statement on the evaluation and management of ventricular arrhythmias in the child with a structurally normal heart. Heart Rhythm. 2014;11:55–78. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
