

Position of scapula and clavicle in acute acromioclavicular joint dislocations: depressed scapula or elevated distal clavicle?
- PMID: 37969526
- PMCID: PMC10638563
- DOI: 10.1016/j.jseint.2023.06.011
Position of scapula and clavicle in acute acromioclavicular joint dislocations: depressed scapula or elevated distal clavicle?
Abstract
Background: Increased coracoclavicular distance due to acute acromioclavicular joint (ACJ) instability is often described as a pseudoelevation of the clavicle due to inferior hanging of the scapula, while the distal clavicle remains in its position. The aim of this study was to analyze whether the elevation of the distal clavicle, depression of the scapula, or both are associated with vertical instability and to evaluate the impact of weighted stress radiographs on the clavicle and scapular position in acute ACJ instabilities.
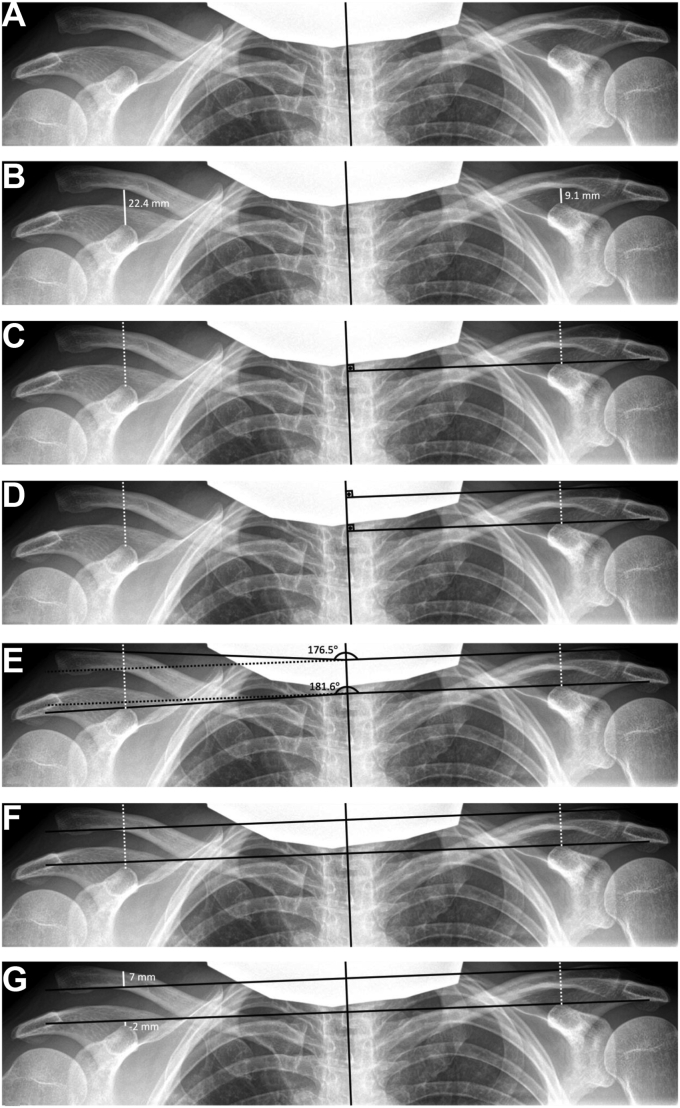
Methods: The cohort consisted of 505 patients (f = 52, m = 453; mean age 46 years) which presented to our emergency department or outpatient clinic and treated in our institution from 2006 to 2019 displaying an acute ACJ injury. The panorama views that displayed at least two vertebraes with their spinous processes were retrospectively evaluated. Two raters assessed the panorama views twice regarding the clavicular and coracoidal angle of both sides in relation to the cervicothoracal spine and the difference in height of both clavicles and coracoids.
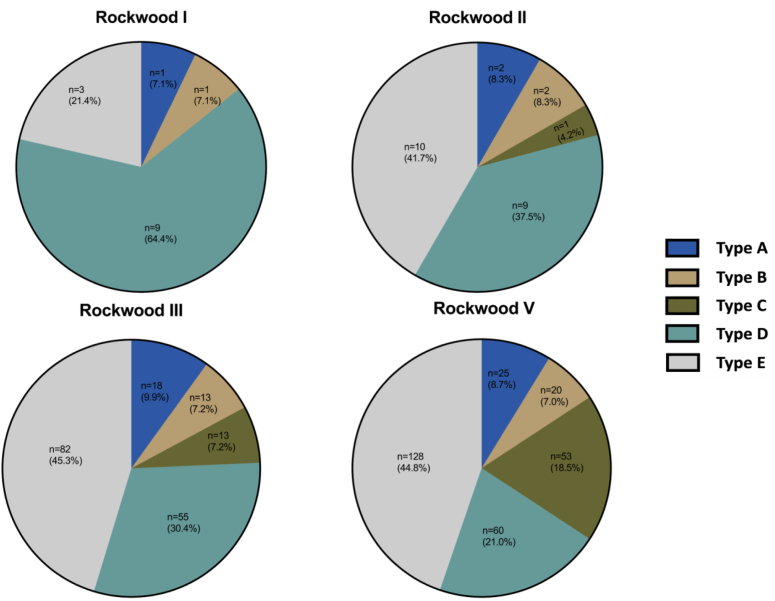
Results: In our cohort, five types of displacement were distinguished: type A, only clavicle is elevated (N = 46); B, only scapula depressed (N = 36); C, the clavicle elevated and the scapula depressed (N = 67); D, both depressed (N = 133); and E, both elevated (N = 223). 123 patients had non-weighted radiographs and 353 patients stress views with 10 kg of axial load, whereas 29 patients had both radiological modalities. Among these 29 patients, a significant increase in coracoclavicular distance difference, clavicle, and scapula height (P < .05, respectively) was observed, when non-weighted radiographs were compared with weighted. A total of 13 shifts could be observed during the Rockwood type comparison of non-weighted radiographs with the weighted: six from Rockwood type II to III, two from type III to V, and five from type V to type III.
Conclusion: Acute injury to the ACJ does not exclusively lead to a depression of the scapula or an elevated distal clavicle but rather leads to various vertical displacement combinations, however mostly to the elevation of both structures possibly due to muscle spasm and pain. Comparing both radiological modalities of the same patients, the routine use of weighted views should be questioned, since often a shift of Rockwood stage can be observed might lead to on the one hand inadequate conservative treatment for underestimated injuries however on the other hand unnecessary surgery for overestimated dislocations.
Keywords: Acute acromioclavicular joint dislocation; Coracoclavicular distance; Non-weighted panorama views; Pseudoelevation of the clavicle; Rockwood classification; Vertical displacement; Weighted panorama views.
© 2023 The Authors.
Figures



References
-
- Allman F.L.J. Fractures and ligamentous injuries of the clavicle and its articulation. JBJS. 1967;49:774. - PubMed
-
- Bearden J.M., Hughston J.C., Whatley G.S. Acromioclavicular dislocation: method of treatment. J Sports Med. 1973;1:5–17. - PubMed
-
- Bossart P.J., Joyce S.M., Manaster B.J., Packer S.M. Lack of efficacy of 'weighted' radiographs in diagnosing acute acromioclavicular separation. Ann Emerg Med. 1988;17:20–24. - PubMed
LinkOut - more resources
Full Text Sources