

Medical Management of Infants With Supraventricular Tachycardia: Results From a Registry and Review of the Literature
- PMID: 37969556
- PMCID: PMC10642123
- DOI: 10.1016/j.cjcpc.2021.09.001
Medical Management of Infants With Supraventricular Tachycardia: Results From a Registry and Review of the Literature
Abstract
Background: Several medication choices are available for acute and prophylactic treatment of refractory supraventricular tachycardia (SVT) in infants. There are almost no controlled trials, and medication choices are not necessarily evidence based. Our objective was to report the effectiveness of management strategies for infant SVT.
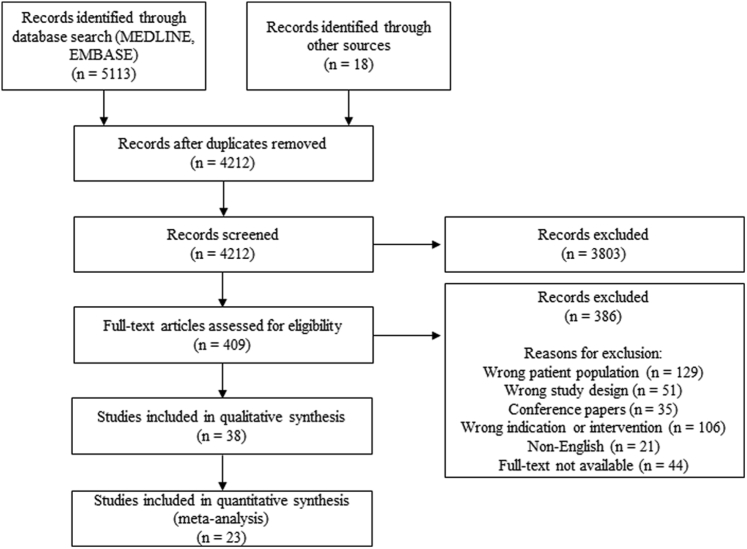
Methods: A registry of infants admitted to hospital with re-entrant SVT and no haemodynamically significant heart disease were prospectively followed at 11 international tertiary care centres. In addition, a systematic review of studies on infant re-entrant SVT in MEDLINE and EMBASE was conducted. Data on demographics, symptoms, acute and maintenance treatments, and outcomes were collected.
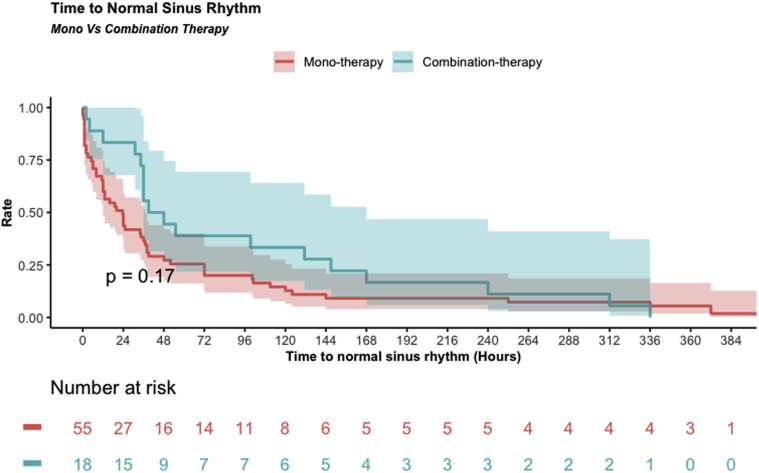
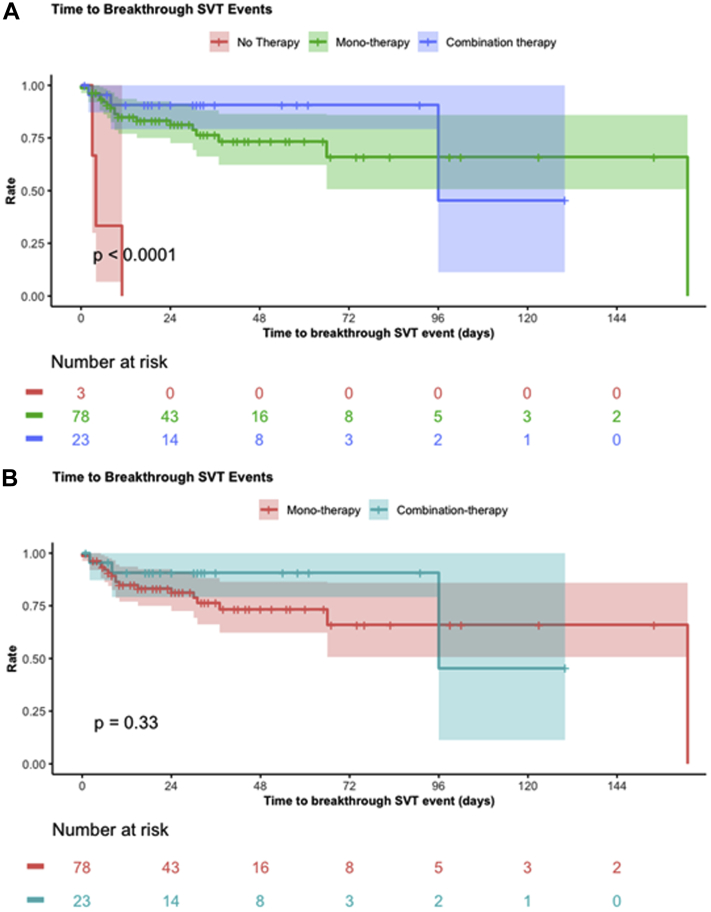
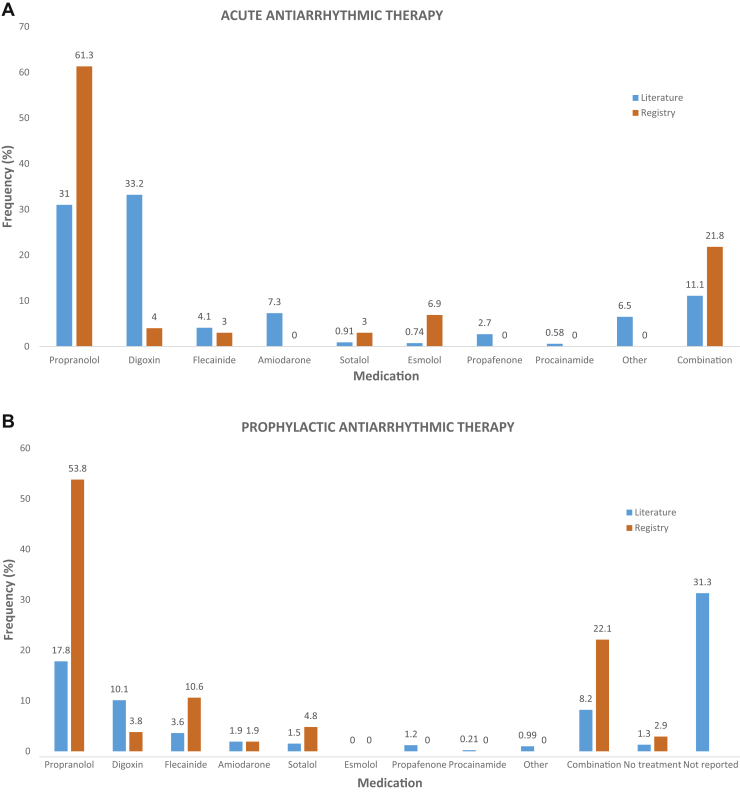
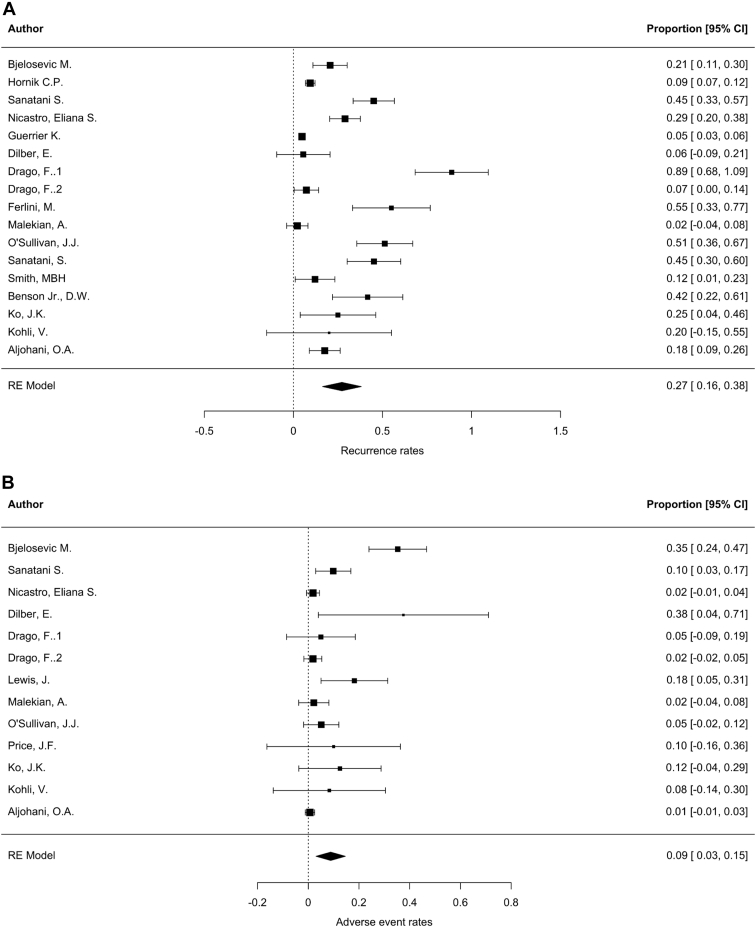
Results: A total of 2534 infants were included: n = 108 from the registry (median age, 9 days [0-324 days], 70.8% male) and n = 2426 from the literature review (median age, 14 days; 62.3% male). Propranolol was the most prevalent acute (61.4%) and maintenance treatment (53.8%) in the Registry, whereas digoxin was used sparingly (4.0% and 3.8%, respectively). Propranolol and digoxin were used frequently in the literature acutely (31% and 33.2%) and for maintenance (17.8% and 10.1%) (P < 0.001). No differences in acute or prophylactic effectiveness between medications were observed. Recurrence was higher in the Registry (25.0%) vs literature (13.4%) (P < 0.001), and 22 (0.9%) deaths were reported in the literature vs none in the Registry.
Conclusion: This was the largest cohort of infants with SVT analysed to date. Digoxin monotherapy use was rare amongst contemporary paediatric cardiologists. There was limited evidence to support one medication over another. Overall, recurrence and mortality rates on antiarrhythmic treatment were low.
Contexte: De nombreux choix de médicaments existent pour le traitement aigu et prophylactique de la tachycardie supraventriculaire (TSV) réfractaire chez les nourrissons. Or, il n’y a presque pas d’essais contrôlés à ce sujet, et les choix de médicaments ne sont pas nécessairement fondés sur des données probantes. Notre objectif était de faire état de l’efficacité des stratégies de prise en charge de la TSV chez les nourrissons.
Méthodologie: Un registre des nourrissons admis à l’hôpital pour une TSV par réentrée, sans cardiopathie d’importance hémodynamique, a été tenu de façon prospective dans 11 centres de soins tertiaires à l’échelle mondiale. De plus, une revue systématique des études sur la TSV par réentrée chez le nourrisson a été effectuée dans MEDLINE et EMBASE. Des données sur les caractéristiques démographiques, les symptômes, les traitements aigus et d’entretien, et les résultats ont été recueillis.
Résultats: Un total de 2 534 nourrissons ont été inclus : n = 108 du registre (âge médian de 9 jours [0-324 jours], 70,8 % de sexe masculin) et n = 2 426 de la revue de la littérature (âge médian de 14 jours; 62,3 % de sexe masculin). Le propranolol était le traitement de soins aigus (61,4 %) et d’entretien (53,8 %) le plus fréquent dans le registre, alors que la digoxine a été utilisée occasionnellement (respectivement dans 4,0 % et 3,8 % des cas). Dans la littérature, le propranolol et la digoxine étaient fréquemment utilisés en soins aigus (31 % et 33,2 %) et en traitement d’entretien (17,8 % et 10,1 %) (p < 0,001). Aucune différence n’a été observée entre les médicaments au chapitre de l’efficacité du traitement de soins aigus ou du traitement prophylactique. Le taux de récurrence était plus élevé dans le registre (25,0 %) que dans la littérature (13,4 %) (p < 0,001), et 22 (0,9 %) décès ont été signalés dans la littérature, mais aucun dans le registre.
Conclusion: Il s’agit de la plus grande cohorte de nourrissons atteints de TSV analysée à ce jour. De nos jours, les cardiologues pédiatriques prescrivent rarement la digoxine en monothérapie. Peu de données probantes favorisent l’utilisation d’un médicament par rapport à l’autre. Dans l’ensemble, les taux de récurrence et de mortalité sous traitement antiarythmique étaient faibles.
© 2021 The Author(s).
Figures
References
-
- Ros S.P., Fisher E.A., Bell T.J. Adenosine in the emergency management of supraventricular tachycardia. Pediatr Emerg Care. 1991;7:222–223. - PubMed
-
- Reyes G., Stanton R., Galvis A.G. Adenosine in the treatment of paroxysmal supraventricular tachycardia in children. Ann Emerg Med. 1992;21:1499–1501. - PubMed
-
- Anand R.G., Rosenthal G.L., Van Hare G.F., Snyder C.S. Is the mechanism of supraventricular tachycardia in pediatrics influenced by age, gender or ethnicity? Congenit Heart Dis. 2009;4:464–468. - PubMed
-
- Ko J.K., Deal B.J., Strasburger J.F., Benson D.W., Jr. Supraventricular tachycardia mechanisms and their age distribution in pediatric patients. Am J Cardiol. 1992;69:1028–1032. - PubMed
-
- Doniger S.J., Sharieff G.Q. Pediatric dysrhythmias. Pediatr Clin North Am. 2006;53:85–105. - PubMed
LinkOut - more resources
Full Text Sources
