

Chest Pain in Cancer Patients: Prevalence of Myocardial Infarction and Performance of High-Sensitivity Cardiac Troponins
- PMID: 37969646
- PMCID: PMC10635894
- DOI: 10.1016/j.jaccao.2023.08.001
Chest Pain in Cancer Patients: Prevalence of Myocardial Infarction and Performance of High-Sensitivity Cardiac Troponins
Abstract
Background: Little is known about patients with cancer presenting with acute chest discomfort to the emergency department (ED).
Objectives: The aim of this study was to assess the prevalence of acute myocardial infarction (AMI), outcomes, and the diagnostic utility of recommended diagnostic tools in this population.
Methods: Patients presenting with chest pain to the ED were prospectively enrolled in an international multicenter diagnostic study with central adjudication. Cancer status was assessed prospectively and additional cancer details retrospectively. Findings were externally validated in an independent multicenter cohort.
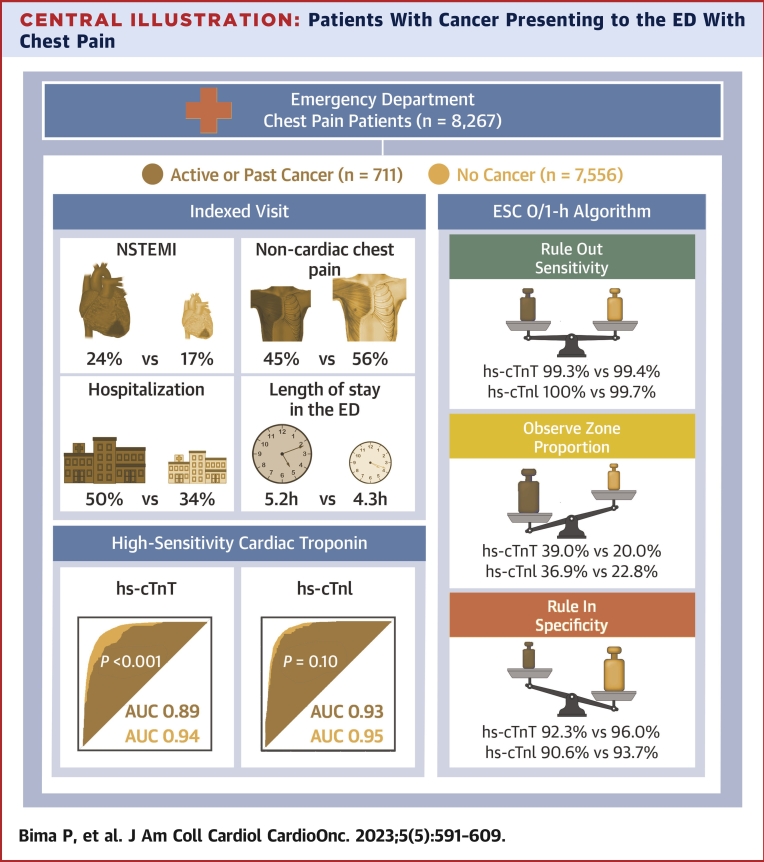
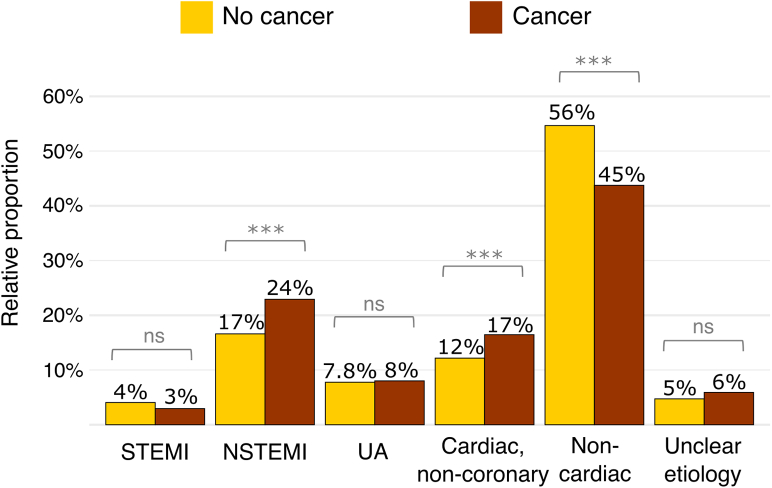
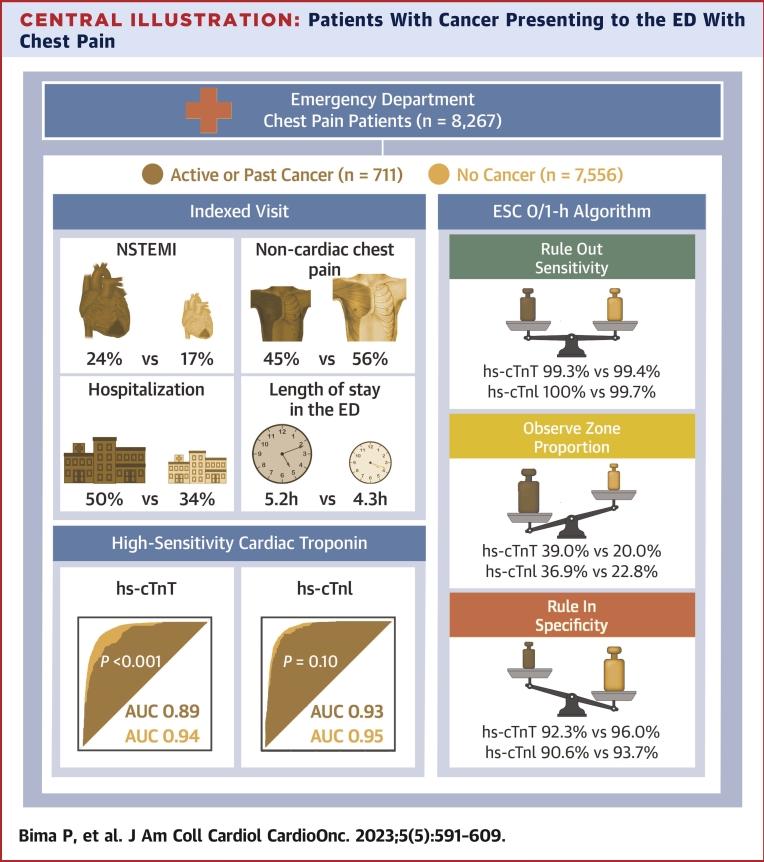
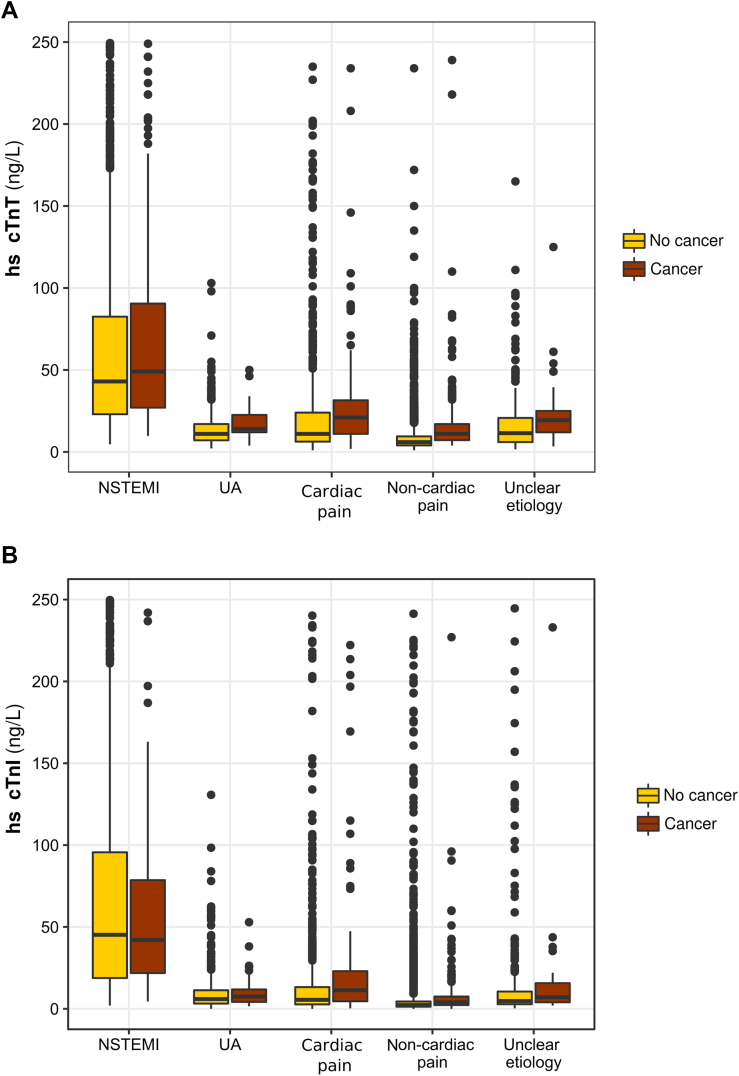
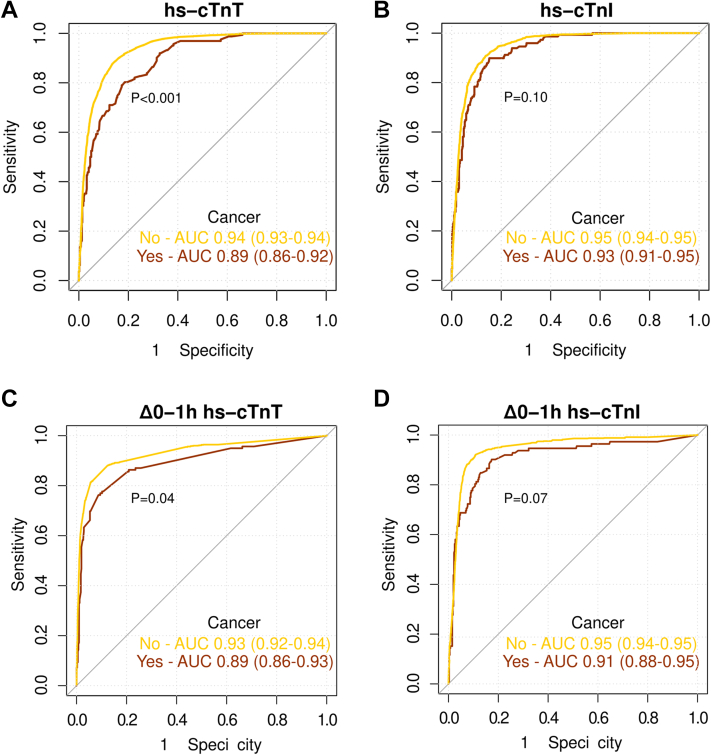
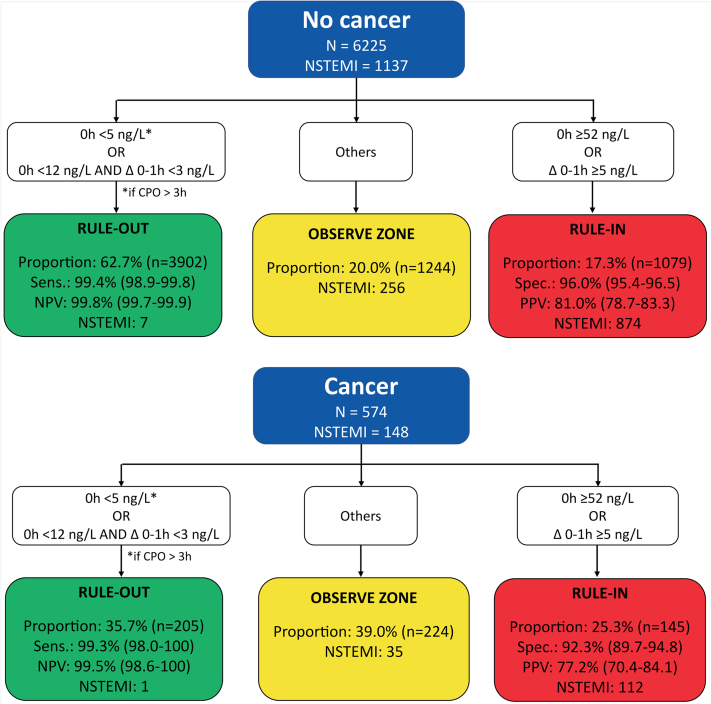
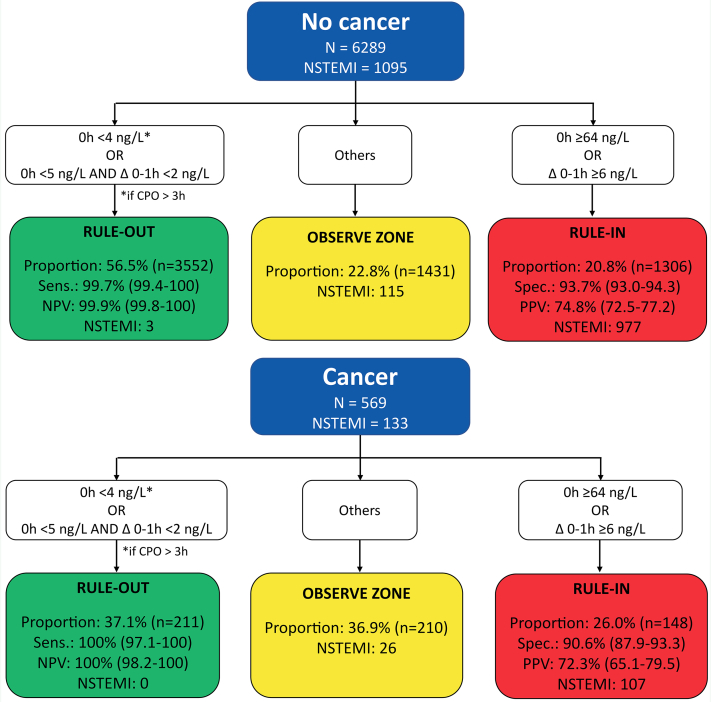
Results: Among 8,267 patients, 711 (8.6%) had cancer. Patients with cancer had a higher burden of cardiovascular risk factors and pre-existing cardiac disease. Total length of stay in the ED (5.2 hours vs 4.3 hours) and hospitalization rate (49.8% vs 34.3%) were both increased in patients with cancer (P < 0.001 for both). Among 8,093 patients eligible for the AMI analyses, those with cancer more often had final diagnoses of AMI (184 of 686 with cancer [26.8%] vs 1,561 of 7,407 without cancer [21.1%]; P < 0.001). In patients with cancer, high-sensitivity cardiac troponin T (hs-cTnT) but not high sensitivity cardiac troponin I (hs-cTnI) concentration had lower diagnostic accuracy for non-ST-segment elevation myocardial infarction (for hs-cTnT, area under the curve: 0.89 [95% CI: 0.86-0.92] vs 0.94 [95% CI: 0.93-0.94] [P < 0.001]; for hs-cTnI, area under the curve: 0.93 [95% CI: 0.91-0.95] vs 0.95 [95% CI: 0.94-0.95] [P = 0.10]). In patients with cancer, the European Society of Cardiology 0/1-hour hs-cTnT and hs-cTnI algorithms maintained very high safety but had lower efficacy, with twice the number of patients remaining in the observe zone. Similar findings were obtained in the external validation cohort.
Conclusions: Patients with cancer have a substantially higher prevalence of AMI as the cause of chest pain. Length of ED stay and hospitalization rates are increased. The diagnostic performance of hs-cTnT and the efficacy of both the European Society of Cardiology 0/1-hour hs-cTnT and hs-cTnI algorithms is reduced. (Advantageous Predictors of Acute Coronary Syndromes Evaluation [APACE] Study; NCT00470587).
Keywords: acute coronary syndrome; biomarkers; cancer survivorship; coronary artery disease; diagnosis; outcomes.
© 2023 The Authors.
Conflict of interest statement
APACE was supported by research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, the European Union, the Cardiovascular Research Foundation Basel, the University Hospital Basel, the University of Basel, Abbott, Beckman Coulter, Roche, Ortho Clinical Diagnostics, Quidel, Siemens, and Singulex. Dr Lopez-Ayala has received research grants from the Swiss Heart Foundation (FF20079 and FF21103); and has received speaker honoraria from Quidel, paid to the institution, outside the submitted work. Dr Nestelberger has received research support from the Swiss National Science Foundation (P400PM_191037/1), the Prof Dr Max Cloëtta Foundation, Margarete und Walter Lichtenstein-Stiftung (3MS1038), and the University Hospital Basel; and has received speaker honoraria and consulting honoraria from B. Braun, Siemens, Beckman Coulter, Bayer, Ortho Clinical Diagnostics, and Orion Pharma, outside the submitted work. Dr Boeddinghaus has received research grants from the University of Basel and the Division of Internal Medicine, the Swiss Academy of Medical Sciences, and the Gottfried and Julia Bangerter-Rhyner-Foundation; and has received speaker honoraria from Siemens, outside the submitted work. Dr Koechlin has received research grants from the University of Basel, the Swiss Academy of Medical Sciences, the Gottfried and Julia Bangerter-Rhyner Foundation, and Freiwillige Akademische Gesellschaft Basel; and has received speaker honoraria from Roche Diagnostics, Abbott, and Siemens, outside the submitted work. Dr Rubini Gimenez has received research grants from the Swiss Heart Foundation and the Swiss National Science Foundation (P400PM_180828); and has received speaker and consulting honoraria from Abbott, Ortho Clinical Diagnostics, Roche, and Siemens, outside the submitted work. Dr Martin-Sanchez has received speaker, advisory, or consulting fees from Novartis, Merck Sharpe & Dohme, Bristol Myers Squibb, Pfizer, The Medicines Company, Otsuka, Thermo Fisher Scientific, Cardiorentis, and Sanofi; and has received research grants from the Spanish Ministry of Health and FEDER, Mapfre, Novartis, Bayer, Merck Sharpe & Dohme, Abbott, and Orion-Pharma, outside the submitted work. Dr Mueller has received research support from the Swiss National Science Foundation, the Swiss Heart Foundation, the KTI, the University Hospital Basel, the University of Basel, Beckman Coulter, Biomerieux, Brahms, Mitsubishi, Novartis, Ortho Clinical, QuAcuidel, Roche, Siemens, Singulex, and Sphingotec; and has received speaker honoraria and consulting honoraria from AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Osler, Novartis, Roche, Siemens, SpinChip, and Singulex, outside the submitted work, and all paid to the institution. Dr Wildi has received funding from Julia und Gottfried Bangerter Stiftung, the University of Basel, the Wesley Medical Research Foundation, the Prince Charles Hospital Foundation, and the University of Queensland, all outside the submitted work. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. The investigated high-sensitivity cardiac troponin assays were donated by the manufacturer, who had no role in the design of the study, the analysis of the data, the preparation of the manuscript, or the decision to submit the manuscript for publication.
Figures
References
-
- Dagenais G.R., Leong D.P., Rangarajan S., et al. Variations in common diseases, hospital admissions, and deaths in middle-aged adults in 21 countries from five continents (PURE): a prospective cohort study. Lancet. 2020;395:785–794. - PubMed
-
- Siegel R.L., Miller K.D., Fuchs H.E., Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72:7–33. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
