

Prostate-specific Antigen Density as a Proxy for Predicting Prostate Cancer Severity: Is There Any Difference between Systematic and Targeted Biopsy?
- PMID: 37970462
- PMCID: PMC10634460
- DOI: 10.4103/sjmms.sjmms_49_23
Prostate-specific Antigen Density as a Proxy for Predicting Prostate Cancer Severity: Is There Any Difference between Systematic and Targeted Biopsy?
Abstract
Background: Prostate cancer screening with prostate-specific antigen (PSA) can result in unnecessary biopsies and overdiagnosis. Alternately, PSA density (PSAD) calculation may help support biopsy decisions; however, evidence of its usefulness is not concrete.
Objective: To evaluate the predictive value of PSAD for clinically significant prostate cancer detection by systematic and MRI-targeted biopsies.
Methods: This prospective study was conducted at two tertiary hospitals in Riyadh, Saudi Arabia, between December 2018 and November 2021. Patients suspected of prostate cancer were subjected to multi-parametric MRI, and for those with positive findings, systematic and targeted biopsies were performed. Clinically non-significant and significant prostate cancer cases were classified based on histopathology-defined ISUP grade or Gleason score. The PSAD was measured using the prostate volume determined by the MRI and categorized into ≤0.15, 0.16-0.20, and >0.20 ng/ml2 subgroups.
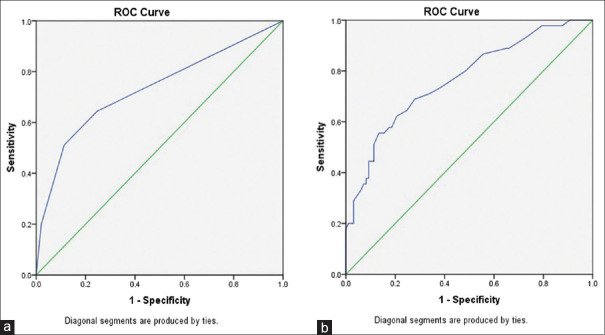
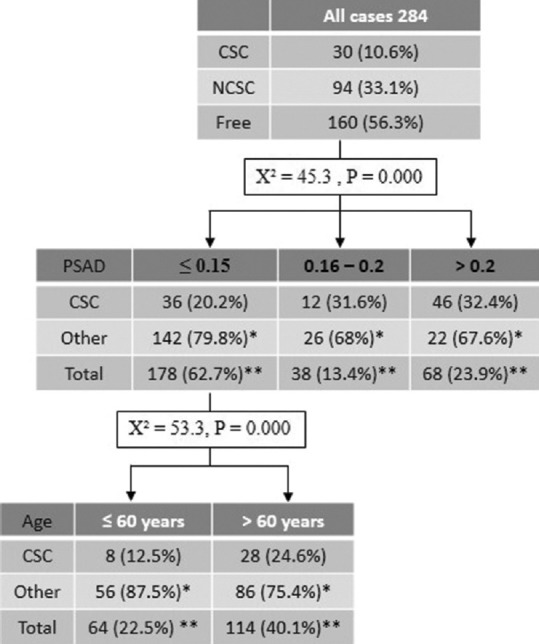
Results: Systematic and targeted biopsies were carried out for 284 patients. The discriminant ability of PSAD is higher in MRI-targeted biopsy compared with systematic biopsy (AUC: 0.77 vs. 0.73). The highest sensitivity (97%) and specificity (87%) were detected at 0.07 ng/ml2 in targeted biopsy. More than half of the clinically significant cases were detected in the >0.2 ng/ml2 PSAD category (systematic: 52.4%; targeted: 51.1%). The CHAID methodology found that the probability of having clinically significant cancer (CSC) in patients with PSAD >0.15 ng/ml2 was more than threefold than that in patients with PSAD ≤0.15 ng/ml2 (64% vs. 20.2%). When considered by age, in PSAD ≤0.15 ng/ml2 subgroup, the percentage of CSC detection rate increased from 20.2% to 24.6% in patients aged ≥60 years.
Conclusion: PSAD has good discriminant power for predicting clinically significant prostate cancer. A cutoff of 0.07 ng/ml2 should be adopted, but should be interpreted with caution and by considering other parameters such as age.
Keywords: Active surveillance; PSA density; advanced prostate cancer; overdiagnosis; prostate-specific antigen; prostatic neoplasm; screening; systematic biopsy; targeted biopsy.
Copyright: © 2023 Saudi Journal of Medicine & Medical Sciences.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
MRI Fusion-Targeted Transrectal Prostate Biopsy and the Role of Prostate-Specific Antigen Density and Prostate Health Index for the Detection of Clinically Significant Prostate Cancer in Southeast Asian Men.J Endourol. 2017 Nov;31(11):1111-1116. doi: 10.1089/end.2017.0485. Epub 2017 Sep 15. J Endourol. 2017. PMID: 28797178
-
Rationale for using serum prostate-specific antigen (PSA) level and PSA density (PSAD) to detect prostatic malignancy in a country with low prostate cancer incidence.Gan To Kagaku Ryoho. 2000 May;27 Suppl 2:563-70. Gan To Kagaku Ryoho. 2000. PMID: 10895211
-
The ability of prostate-specific antigen (PSA) density to predict an upgrade in Gleason score between initial prostate biopsy and prostatectomy diminishes with increasing tumour grade due to reduced PSA secretion per unit tumour volume.BJU Int. 2012 Jul;110(1):36-42. doi: 10.1111/j.1464-410X.2011.10681.x. Epub 2011 Nov 15. BJU Int. 2012. PMID: 22085203
-
The Use of Multiparametric Magnetic Resonance Imaging for Follow-up of Patients Included in Active Surveillance Protocol. Can PSA Density Discriminate Patients at Different Risk of Reclassification?Clin Genitourin Cancer. 2020 Dec;18(6):e698-e704. doi: 10.1016/j.clgc.2020.04.006. Epub 2020 May 4. Clin Genitourin Cancer. 2020. PMID: 32493676
-
Personalized prostate biopsy protocols: enhancing cancer detection through tailored approaches-a narrative review.Transl Androl Urol. 2025 Mar 30;14(3):831-840. doi: 10.21037/tau-24-619. Epub 2025 Mar 26. Transl Androl Urol. 2025. PMID: 40226054 Free PMC article. Review.
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–49. - PubMed
-
- Culp MB, Soerjomataram I, Efstathiou JA, Bray F, Jemal A. Recent global patterns in prostate cancer incidence and mortality rates. Eur Urol. 2020;77:38–52. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous