

Effect on the Quality of Life of Patients with Heart Failure and Reduced/Preserved Ejection Fraction Using Sacubitril/Valsartan
- PMID: 37971045
- PMCID: PMC10519244
- DOI: 10.36660/abc.20220611
Effect on the Quality of Life of Patients with Heart Failure and Reduced/Preserved Ejection Fraction Using Sacubitril/Valsartan
Abstract
Background: Heart failure (HF) management has markedly improved, but a clinically meaningful improvement in functional capacity and quality of life is perhaps more important for patients than living longer.
Objective: This study aimed to review the improvement in quality of life with sacubitril/valsartan in patients with HF and reduced/preserved ejection fraction (EF) from prospective clinical trials.
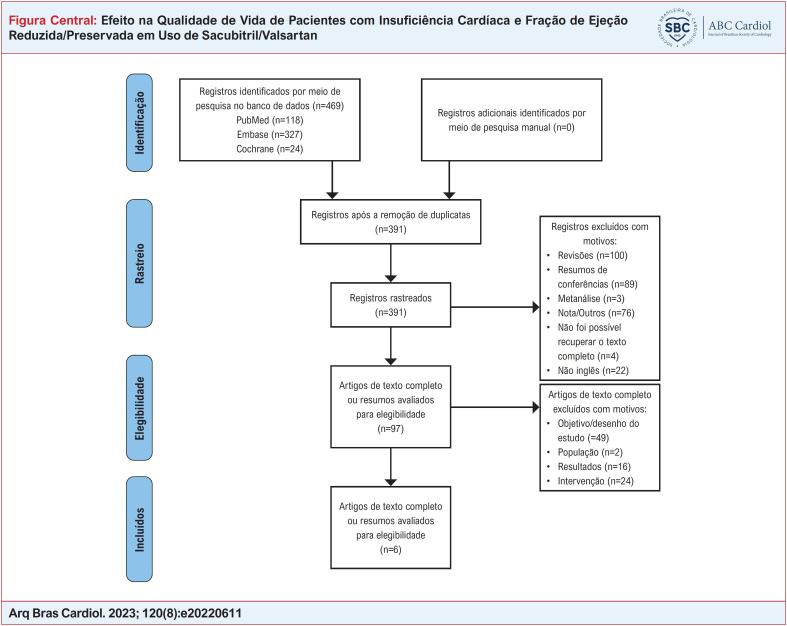
Methods: PubMed, Embase, and the Cochrane Library were searched for randomized controlled trials (RCTs) and prospective cohort studies published from inception to July 2021. A total of 6 clinical trials and 16854 patients with HF were included. The primary outcome was the change from baseline in KCCQ clinical summary score. The secondary outcomes were scores in other domains of KCCQ, the occurrence of serious adverse events (AEs), and overall mortality. P-values <0.05 were considered statistically significant.
Results: Treatment of sacubitril/valsartan showed significantly higher KCCQ-CSS compared to the control (WMD=0.975, 95% CI: 0.885, 1.064, p<0.001; I2=94.8%, pheterogeneity<0.001). A significant decrease in the mortality rate was observed in the sacubitril/valsartan group compared to the control group (RR=0.895, 95%CI:0.831, 0.965, p=0.004; I2=43.6%, pheterogeneity=0.150). Nevertheless, no significant reduction in the occurrence of serious AEs was found among HF patients treated with sacubitril/valsartan compared to the control group (RR=0.950, 95%CI: 0.879, 1.027, p<0.001; I2=68.1%, pheterogeneity=0.024).
Conclusions: Our study demonstrated that sacubitril/valsartan might significantly improve the HRQL compared to other treatments according to the results in KCCQ-CSS and some subdomains in the KCCQ index during the follow-up in patients with HF.
Fundamento: O manejo da insuficiência cardíaca (IC) tem melhorado acentuadamente, mas uma melhora clinicamente significativa na capacidade funcional e na qualidade de vida talvez seja mais importante para os pacientes do que viver mais.
Objetivo: Este estudo teve como objetivo revisar a melhora na qualidade de vida com sacubitril/valsartan em pacientes com IC e fração de ejeção (FE) reduzida/preservada a partir de ensaios clínicos prospectivos.
Métodos: PubMed, Embase e Cochrane Library foram pesquisados em busca de ensaios clínicos randomizados (ECRs) e estudos de coorte prospectivos publicados desde o início até julho de 2021. Um total de 6 ensaios clínicos e 16.854 pacientes com IC foram incluídos. O desfecho primário foi a alteração da linha de base na pontuação do resumo clínico do KCCQ. Os desfechos secundários foram pontuações em outros domínios do KCCQ, ocorrência de eventos adversos graves (EAs) e mortalidade geral. Valores de p < 0,05 foram considerados estatisticamente significativos.
Resultados: O tratamento de sacubitril/valsartan mostrou KCCQ-CSS significativamente maior em comparação com o controle (DMP=0,975, IC 95%:0,885, 1,064, p<0,001; I2=94,8%, pheterogeneidade<0,001). Uma diminuição significativa na taxa de mortalidade foi observada no grupo sacubitril/valsartan em comparação com o grupo controle (RR=0,895, IC 95%: 0,831, 0,965, p=0,004; I2=43,6%, pheterogeneidade=0,150). No entanto, nenhuma redução significativa na ocorrência de EAs graves foi encontrada entre pacientes com IC tratados com sacubitril/valsartan em comparação com o grupo controle (RR=0,950, IC 95%: 0,879, 1,027, p<0,001; I2=68,1%, pheterogeneidade= 0,024).
Conclusões: Nosso estudo demonstrou que o sacubitril/valsartan pode melhorar significativamente a QVRS em comparação com outros tratamentos de acordo com os resultados do KCCQ-CSS e alguns subdomínios do índice KCCQ durante o acompanhamento em pacientes com IC.
Conflict of interest statement
Potencial conflito de interesse
Não há conflito com o presente artigo
Figures









References
-
- Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJ, Ponikowski P, Poole-Wilson PA, et al. ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in Collaboration with the Heart Failure Association of the ESC (HFA) and Endorsed by the European Society of Intensive Care Medicine (ESICM) Eur J Heart Fail. 2008;10(10):933–989. doi: 10.1016/j.ejheart.2008.08.005. - DOI - PubMed
-
- Juenger J, Schellberg D, Kraemer S, Haunstetter A, Zugck C, Herzog W, et al. Health Related Quality of Life in Patients with Congestive Heart Failure: Comparison with Other Chronic Diseases and Relation to Functional Variables. Heart. 2002;87(3):235–241. doi: 10.1136/heart.87.3.235. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
