

Incidence of Recurrence and Time to Recurrence in Stage I to III Colorectal Cancer: A Nationwide Danish Cohort Study
- PMID: 37971197
- PMCID: PMC10654928
- DOI: 10.1001/jamaoncol.2023.5098
Incidence of Recurrence and Time to Recurrence in Stage I to III Colorectal Cancer: A Nationwide Danish Cohort Study
Abstract
Importance: Management of colorectal cancer (CRC) has been updated continuously over the past 2 decades. While the combination of these initiatives has had implications for improved survival, the implications for rates of recurrence remain unexplored.
Objective: To ascertain the rates of recurrence and describe time to recurrence within 5 years of surgery with curative intent for stages I to III CRC.
Design, setting, and participants: This cohort study used the Danish Colorectal Cancer Group Database to identify patients with Union for International Cancer Control (UICC) stages I to III CRC who underwent primary surgery between January 1, 2004, and December 31, 2019. They were followed up until recurrence (event), death (competing event), diagnosis of a second cancer (competing event), emigration (censoring event), 5 years postoperatively (censoring event), or January 1, 2023 (censoring event), whichever came first. Recurrence status was ascertained through individual-level linked data from the Danish Cancer Registry, Danish National Patient Registry, and Danish Pathology Registry using a validated algorithm. Data were analyzed from January 1 to August 8, 2023.
Exposure: Primary surgery performed during 3 calendar periods (2004-2008, 2009-2013, and 2014-2019) stratified by tumor site (colon or rectum) and UICC stage (I, II, and III).
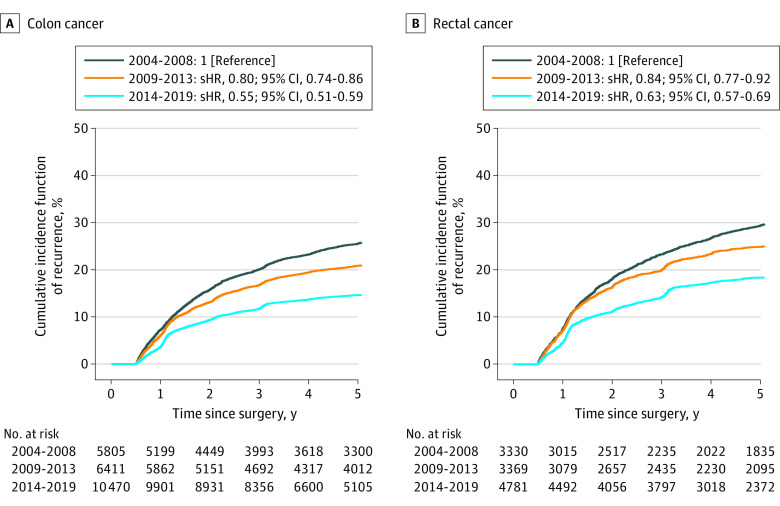
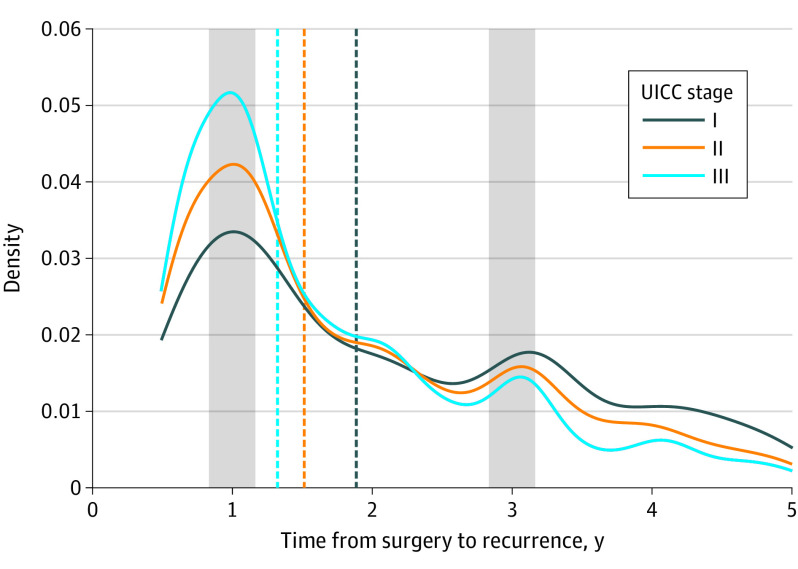
Main outcomes and measures: Stage-specific 5-year recurrence reported as the cumulative incidence function (CIF) of recurrence, the association between calendar period of primary surgery and recurrence risk reported as subdistribution hazard ratios (sHRs), and the time from surgery to recurrence.
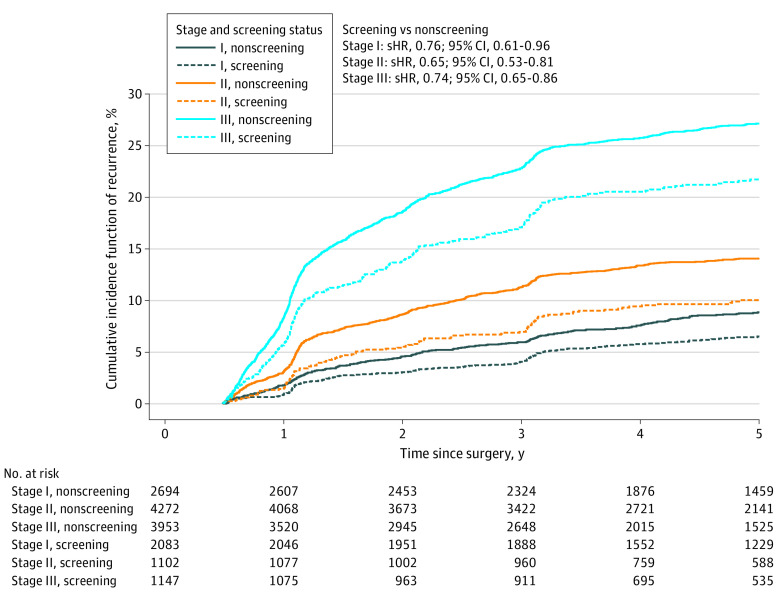
Results: Of the 34 166 patients with UICC stages I to III CRC (median [IQR] age, 70 [62-77] years); 18 552 males [54.3%]) included in the study, 7027 developed recurrence within 5 years after the primary surgery. For colon cancer, the 5-year CIF of recurrence decreased over the 3 calendar periods from 16.3% to 6.8% for UICC stage I, from 21.9% to 11.6% for UICC stage II, and from 35.3% to 24.6% for UICC stage III colon cancer. For rectal cancer, the 5-year CIF decreased over the 3 periods from 19.9% to 9.5% for stage I, from 25.8% to 18.4% for stage II, and from 38.7% to 28.8% for stage III disease. Patients with stage III disease had a shorter time from surgery to recurrence compared with those with stage I disease (time ratio stage III vs stage I = 0.30; 95% CI, 0.28-0.32). Cancers detected through screening were associated with lower stage-adjusted risks of recurrence (sHR, 0.81; 95% CI, 0.73-0.91) compared with cancers not detected through screening.
Conclusions and relevance: In this cohort of patients with CRC, the risk of recurrence decreased in patients with stages I to III disease during the study period. Cancer detection by screening was associated with an even lower risk of recurrence. Time to recurrence differed according to UICC stage. Because the risk of recurrence was so low in selected patient groups, future research is warranted to explore risk-stratified surveillance protocols in patients with CRC.
Conflict of interest statement
Figures
Comment in
-
Moving Toward Personalized Colorectal Cancer Follow-Up Care.JAMA Oncol. 2024 Jan 1;10(1):29-31. doi: 10.1001/jamaoncol.2023.5072. JAMA Oncol. 2024. PMID: 37971198 No abstract available.
References
-
- Shah MA, Renfro LA, Allegra CJ, et al. . Impact of patient factors on recurrence risk and time dependency of oxaliplatin benefit in patients with colon cancer: analysis from modern-era adjuvant studies in the Adjuvant Colon Cancer End Points (ACCENT) Database. J Clin Oncol. 2016;34(8):843-853. doi:10.1200/JCO.2015.63.0558 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
